J Lung Cancer.
2011 Dec;10(2):94-101. 10.6058/jlc.2011.10.2.94.
Inconclusive Result from CT Guided Transthoracic Needle Aspiration and Biopsy: Affecting Factors and Final Outcome
- Affiliations
-
- 1Department of Internal Medicine, Lung Institute of Medical Research Center, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Internal Medicine and Lung Institute of Medical Research Center, Hallym University Sacred Heart Hospital, Anyang, Korea.
- 3Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Internal Medicine, Lung Institute of Medical Research Center, Seoul National University Bundang Hospital, Seongnam, Korea. jhlee7@snubh.org
- KMID: 2005740
- DOI: http://doi.org/10.6058/jlc.2011.10.2.94
Abstract
- PURPOSE
Inconclusive results from computed tomography (CT)-guided transthoracic needle aspiration and biopsy (TNAB) performed for lung lesions presents a clinical dilemma. The purpose of this study was to determine the factors affecting an inconclusive result from a CT guided TNAB, and to evaluate the final outcomes of these inconclusive results.
MATERIALS AND METHODS
The medical records and radiologic features of 331 patients with lung lesion who received CT guided TNAB were analyzed retrospectively. The results of the TNAB were classified as conclusive (malignancy or specific benign diagnosis) or inconclusive (nonspecific benign or nondiagnostic).
RESULTS
Of the 331 cases, 269 (81.3%) were diagnosed as a malignancy (210) or a specific benign lesion (59) after the first TNAB. The remaining 62 (18.7%) were inconclusive. Benign disease, a lesion size < or =15 mm, and morphology of the consolidation type were features significantly correlated with inconclusive results. Of these 62 inconclusive cases a second TNAB was performed in 23, and conclusive diagnoses were obtained in 19 (82.6%). Surgery or radiographic follow up was done in other cases. Finally, among the 62 inconclusive results on the first CT guided TNAB, 16 lesions were diagnosed as malignant, 26 were classified as specific benign disease, and the remaining 20 were defined as nonspecific inflammation. Age over 50 and morphology of a nodule or a mass type were significantly correlated with a malignancy in these 62 cases with inconclusive results on the first TNAB.
CONCLUSION
A final diagnosis of benign disease was significantly higher after the CT guided TNAB was inconclusive for lesions < or =15 mm that had consolidation type morphology. Despite the application of core biopsy procedures, there continue to be appreciable numbers of inconclusive results after the first CT guided TNAB. A repeat CT guided TNAB had a high diagnostic yield in these cases and therefore should be considered for cases with inconclusive results.
Figure
-
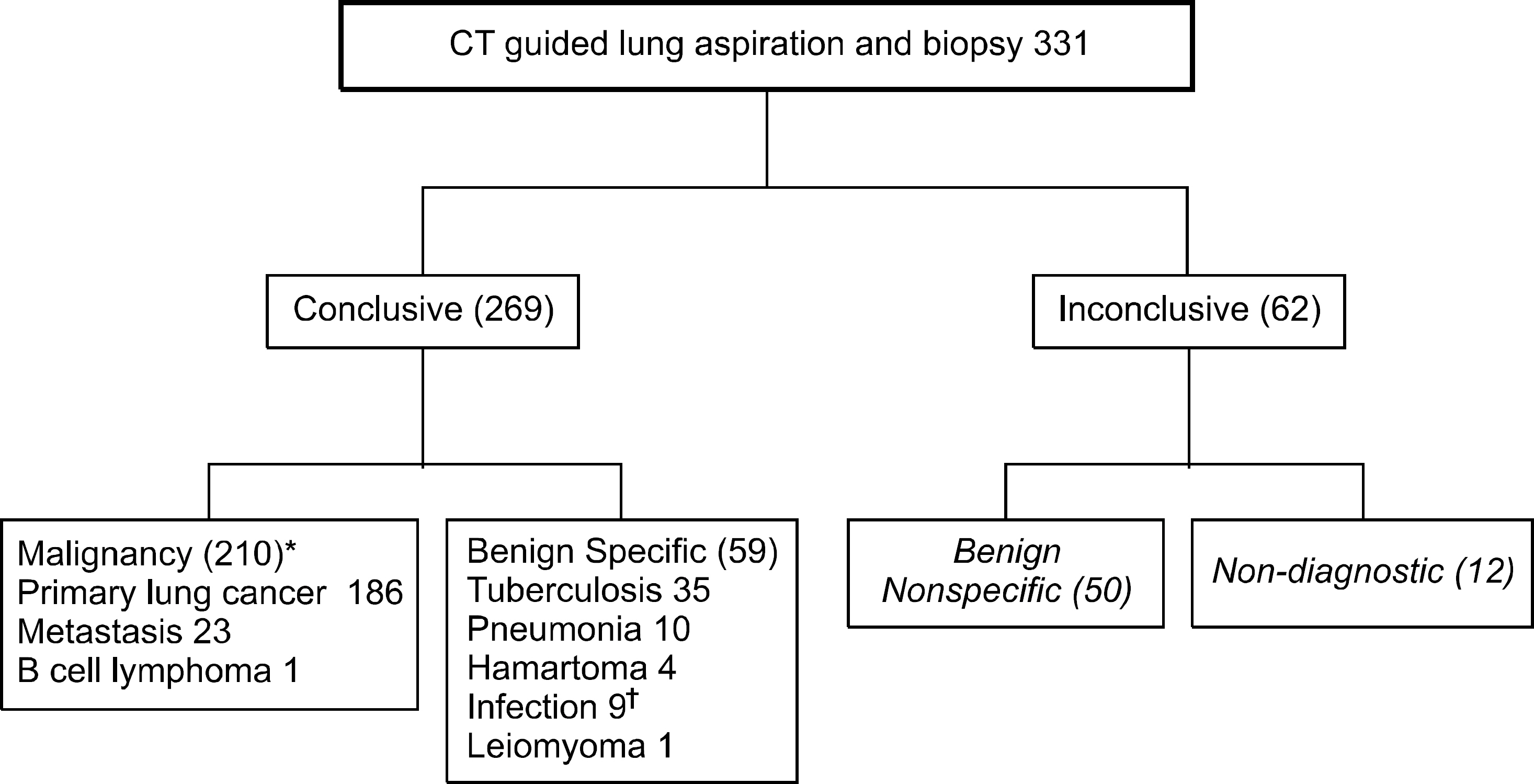
Fig. 1. Diagnostic algorithm of 331 patients with pulmonary lesions after a first trial of transthoracic needle aspiration and biopsy. ∗In-cluding one false positive case of adenocarcinoma which proved to be tuberculosis after surgery, † Paragonimiasis, actinomycosis, non-tuberculous mycobacterium in-cluded.
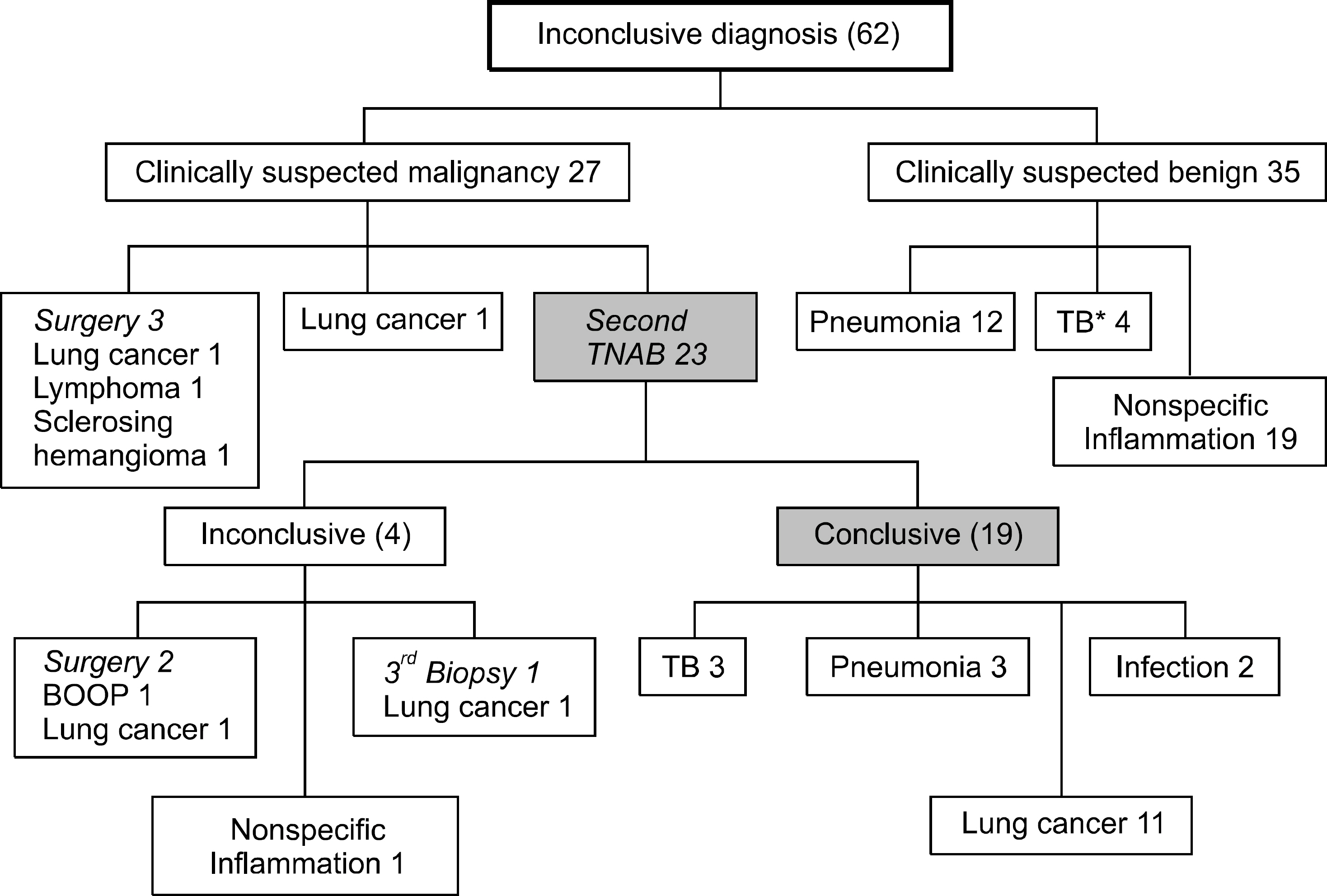
Fig. 2. Diagnostic algorithm of lung lesions with an inconclusive first CT guided TNAB result. TB: tuberculosis, BOOP: bronchiolitis obliterans with organizing pneumonia.
Reference
-
1. Murphy JM, Gleeson FV, Flower CD. Percutaneous needle biopsy of the lung and its impact on patient management. World J Surg. 2001; 25:373–379.
Article2. Schreiber G, McCrory DC. Performance characteristics of different modalities for diagnosis of suspected lung cancer: summary of published evidence. Chest. 2003; 123(1 Suppl):115S–128S.3. Laurent F, Latrabe V, Vergier B, Montaudon M, Vernejoux JM, Dubrez J. CT-guided transthoracic needle biopsy of pulmonary nodules smaller than 20 mm: results with an automated 20-gauge coaxial cutting needle. Clin Radiol. 2000; 55:281–287.4. Klein JS, Salomon G, Stewart EA. Transthoracic needle biopsy with a coaxially placed 20-gauge automated cutting needle: results in 122 patients. Radiology. 1996; 198:715–720.
Article5. Tsukada H, Satou T, Iwashima A, Souma T. Diagnostic accuracy of CT-guided automated needle biopsy of lung nodules. AJR Am J Roentgenol. 2000; 175:239–243.
Article6. Yeow KM, Tsay PK, Cheung YC, Lui KW, Pan KT, Chou AS. Factors affecting diagnostic accuracy of CT-guided coaxial cutting needle lung biopsy: retrospective analysis of 631 procedures. J Vasc Interv Radiol. 2003; 14:581–588.
Article7. Arslan S, Yilmaz A, Bayramgü rler B, Uzman O, Nver E, Akkaya E. CT- guided transthoracic fine needle aspiration of pulmonary lesions: accuracy and complications in 294 patients. Med Sci Monit. 2002; 8:CR493–CR497.8. Manhire A, Charig M, Clelland C, et al. Guidelines for radio-logically guided lung biopsy. Thorax. 2003; 58:920–936.
Article9. Lacasse Y, Wong E, Guyatt GH, Cook DJ. Transthoracic needle aspiration biopsy for the diagnosis of localised pulmonary lesions: a meta-analysis. Thorax. 1999; 54:884–893.
Article10. Klein JS, Zarka MA. Transthoracic needle biopsy. Radiol Clin North Am. 2000; 38:235–266.
Article11. Ghaye B, Dondelinger RF. Imaging guided thoracic inter-ventions. Eur Respir J. 2001; 17:507–528.
Article12. Westcott JL. Percutaneous transthoracic needle biopsy. Radiology. 1988; 169:593–601.
Article13. Westcott JL, Rao N, Colley DP. Transthoracic needle biopsy of small pulmonary nodules. Radiology. 1997; 202:97–103.
Article14. Wallace MJ, Krishnamurthy S, Broemeling LD, et al. CT- guided percutaneous fine-needle aspiration biopsy of small (< or =1-cm) pulmonary lesions. Radiology. 2002; 225:823–828.15. Greif J, Marmor S, Schwarz Y, Staroselsky AN. Percutaneous core needle biopsy vs. fine needle aspiration in diagnosing benign lung lesions. Acta Cytol. 1999; 43:756–760.
Article16. Savage C, Walser EM, Schnadig V, Woodside KJ, Ustuner E, Zwischenberger JB. Transthoracic image-guided biopsy of lung nodules: when is benign really benign? J Vasc Interv Radiol. 2004; 15:161–164.
Article17. Meyer CA. “Transthoracic needle aspiration biopsy of benign and malignant lung lesions”–a commentary. AJR Am J Roentgenol. 2007; 188:891–893.
Article18. Quint LE, Kretschmer M, Chang A, Nan B. CT-guided thoracic core biopsies: value of a negative result. Cancer Imaging. 2006; 6:163–167.
Article19. Lee IJ, Bae YA, Kim DG, et al. Percutaneous needle aspiration biopsy (PCNAB) of lung lesions: 5 years results with focusing on repeat PCNAB. Eur J Radiol. 2010; 73:551–554.
Article20. Khouri NF, Stitik FP, Erozan YS, et al. Transthoracic needle aspiration biopsy of benign and malignant lung lesions. AJR Am J Roentgenol. 1985; 144:281–288.
Article21. Bungay HK, Adams RF, Morris CM, Haggett PJ, Traill ZC, Gleeson FV. Cutting needle biopsy in the diagnosis of clinic-ally suspected non-carcinomatous disease of the lung. Br J Radiol. 2000; 73:349–355.
Article22. Hirose T, Mori K, Machida S, Tominaga K, Yokoi K, Adachi M. Computed tomographic fluoroscopy-guided transthoracic needle biopsy for diagnosis of pulmonary nodules. Jpn J Clin Oncol. 2000; 30:259–262.
Article23. MacMahon H, Austin JH, Gamsu G, et al. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology. 2005; 237:395–400.
Article24. Oh JY, Kwon SY, Yoon HI, et al. Clinical significance of a solitary ground-glass opacity (GGO) lesion of the lung detected by chest CT. Lung Cancer. 2007; 55:67–73.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of Repeated Endoscopic Ultrasound-Guided Fine Needle Aspiration for Inconclusive Initial Cytology Result
- Painful Percutaneous Transthoracic Needle Biopsy of Schwannoma: A Case Report
- Analysis of the result and merit of computed tomography guided percutaneous needle aspiration biopsy of focal lung lesion
- Fine-Needle Biopsy: Should This Be the First Choice in Endoscopic Ultrasound-Guided Tissue Acquisition?
- Transthoracic Fine Needle Aspiration Biopsy: Diagnostic Rate and Complications in 1000 Cases
