Cervical Spondylolysis with Dysplasia: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Yonsei University, Wonju College of Medicine, Wonju, Korea. par73@yonsei.ac.kr
- KMID: 2003116
- DOI: http://doi.org/10.4184/jkss.2009.16.3.210
Abstract
- Cervical spondylolysis is defined as a corticated cleft between the superior and inferior articular facets of the articular pillar, which is the cervical equivalent of pars interarticularis in the lumbar spine. It is very important to avoid confusion with more clinically significant abnormalities, such as fracture or dislocation. This case report describes bilateral spondylolysis and associated dysplasia of C6. We describe the radiographic presentation of this anomaly, stressing the importance of computed tomography and magnetic resonance imaging for a correct diagnosis. A review of the literature on this interesting abnormality and a complete differential diagnosis are presented.
Keyword
Figure
-
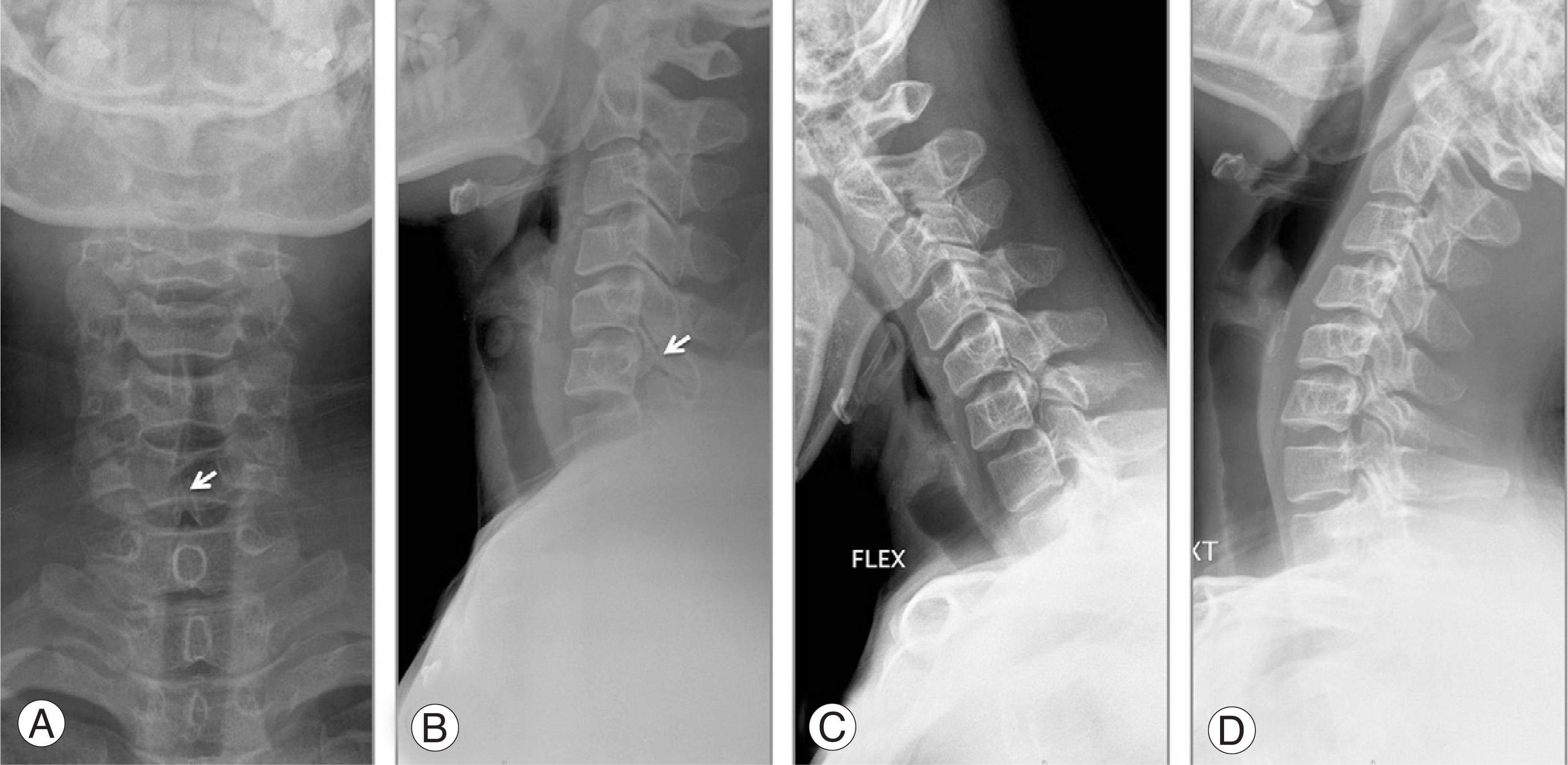
Fig. 1. (A) Anteroposterior radiograph of the cervical spine showing spina bifida occulta at C6. (B) Lateral radiograph revealing a well-corticated defect (arrow) between the superior and inferior articular pillars, dysplastic changes of the facet. (C, D) Flexion and extension views no evidences of instability.

Fig. 2. (A) Sagittal Computed tomography scan showing a well-corticated clefts at facet joint (arrow). (B) Axial computed tomography scan at the level of the pedicle of C6 revealing a well-corticated clefts (arrows) and spina bifida(arrowhead).

Fig. 3. (A) Sagittal T-2weighted magnetic resonance image showing a well-corticated clefts (arrow). (B) Axial T-2 weighted magnetic resonance image showing the spondylolytic defects (arrow). (C) Fat suppression image views no evidence of acute injury.
Cited by 1 articles
-
Multilevel Thoracolumbar Spondylolysis with Spondylolisthesis at L4 on L5
Whoan Jeang Kim, Young Dong Song, Won Sik Choy
Clin Orthop Surg. 2015;7(3):410-413. doi: 10.4055/cios.2015.7.3.410.
Reference
-
1). Forsberg DA, Martinez S, Vogler JB 3rd, Wiener MD. Cervical spondylolysis: imaging findings in 12 patients. AJR Am J Roentgenol. 1990; 154:751–755.
Article2). Hinton MA, Harris MB, King AG. Cervical spondylolysis. Report of two cases. Spine. 1993; 18:1369–1372.3). Morvan G, Busson J, Frot B, Nahum H. Cervical spondylolysis. 7 cases. Review of the literature. J Radiol. 1984; 65:259–266.4). Perlman R, Hawes LE. Cervical spondylolisthesis. J Bone Joint Surg Am. 1951; 33:1012–1013.
Article5). Jeyapalan K, Chavda SV. Case report 868. Congenital bilateral spondylolysis and spondylolisthesis of the fourth cervical vertebra. Skeletal Radiol. 1994; 23:580–582.6). Redla S, Sikdar T, Saifuddin A, Taylor BA. Imaging features of cervical spondylolysis–with emphasis on MR appearances. Clin Radiol. 1999; 54:815–820.7). Oueslati S, Zaouia K, Chelli M. Cervical spondylolysis: a case report. Acta Orthop Belg. 2006; 72:511–516.8). Poggi JJ, Martinez S, Hardaker WT Jr, Richardson WJ. Cervical spondylolysis. J Spinal Disord. 1992; 5:349–356.
Article9). Forsberg DA, Martinez S, Vogler JBⅢ, Wiener MD. Cervical spondylolysis: imaging findings in 12 patients. AJR Am J Roentgenol. 1990; 154:751–755.
Article10). Johansen JG, McCarty DJ, Haughton VM. Retrosomat-ic clefts: computed tomographic appearance. Radiology. 1983; 148:447–448.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cervical Spondylolysis in Child with Four Levels of Simultaneous Involvement: A Case Report
- Cervical Spondylolysis: Report of Two Cases
- Asymptomatic Cervical Isthmic Spondylolisthesis and Associated Occult Spinal Bifida: A Case Report
- Utilization of Three-dimensional Reconstruction Computed Tomography as a Diagnostic Tool for Adult Unilateral Primary Cervical Spondylolysis: Report of Two Cases
- Two Consecutive Levels of Unilateral Cervical Spondylolysis on Opposite Sides
