Radiologic Analysis of Postoperative Sagittal Plane Correction in Lumbar Degenerative Kyphosis (LDK)
- Affiliations
-
- 1Department of Orthopaedic Surgery, Eulji University School of Medicine, Korea. jwkang@eulji.ac.kr
- 2Daejeon Veterans Hospital, Korea.
- 3Hongseong Medical Center, Korea.
- 4Gimcheon Jeil Hospital, Korea.
- KMID: 2003112
- DOI: http://doi.org/10.4184/jkss.2009.16.3.177
Abstract
- STUDY DESIGN: This is a retrospective study OBJECTIVES: We radiologically analyzed the correction of the sagittal imbalance and the proximal fusion level to prevent correction loss and the usefulness of iliac screws in LDK. SUMMARY OF THE LITERATURE REVIEW: Complications can be encountered during fixation and fusion as most of the LDK patients are aged, and the osteoporosis that causes fixation loss is known to affect the loss of correction.
MATERIALS AND METHODS
We analyzed the cause of correction loss among 35 patients who underwent surgery and who were followed up for at least 1 year. All the patients had performed gait analysis before operation. The operative techniques were pedicle subtraction osteotomy and fixation to S1. For analyzing causes of correction loss, we analyzed the degrees of lumbar lordosis for the sagittal correction and the degrees of the preoperative thoracolumbar kyphosis for the proximal fusion range. For analyzing the usefulness of iliac screws, the subjects were divided into two groups: 1) the -iliac screw (23cases) group for the patients who were fixed without iliac screws and 2) the +iliac screw (12cases) group for the patients who were fixed with iliac screws.
RESULTS
There were no patients who had marked anterior pelvic tilt. It is important to correct the lumbar lordosis over 20degrees compared with the preoperative thoracic kyphosis. There are 10 cases of preoperative thoracolumbar kyphosis > or = 10degrees and 25 cases of preoperative thoracolumbar kyphosis < 10degrees of the total 35 cases. Among 10 cases of preoperative thoracolumbar kyphosis > or = 10degrees, 4 cases that were fixed to T10 had no sagittal correction loss, and 2 of the 6 cases that were fixed to T11 or T12 had sagittal correction loss. For the 25 cases of preoperative thoracolumbar kyphosis < 10degrees, 5 cases that were fixed to T10 had no sagittal correction loss and 1 of the 20 cases that were fixed to T11 or T12 had sagittal correction loss (p<0.05). 6 cases (26%) in the -iliac screw group (23 cases total) and 1 case (8%) in the +iliac screw (12 cases total) showed sagittal correction loss (p<0.05).
CONCLUSIONS
It is important to make the postoperative lumbar lordosis over 20degrees compared with the preoperative thoracic kyphosis for correcting sagittal imbalance, to decide on the proximal fixation level according to the preoperative thoracolumbar kyphosis and to fix with iliac screws.
Figure
-
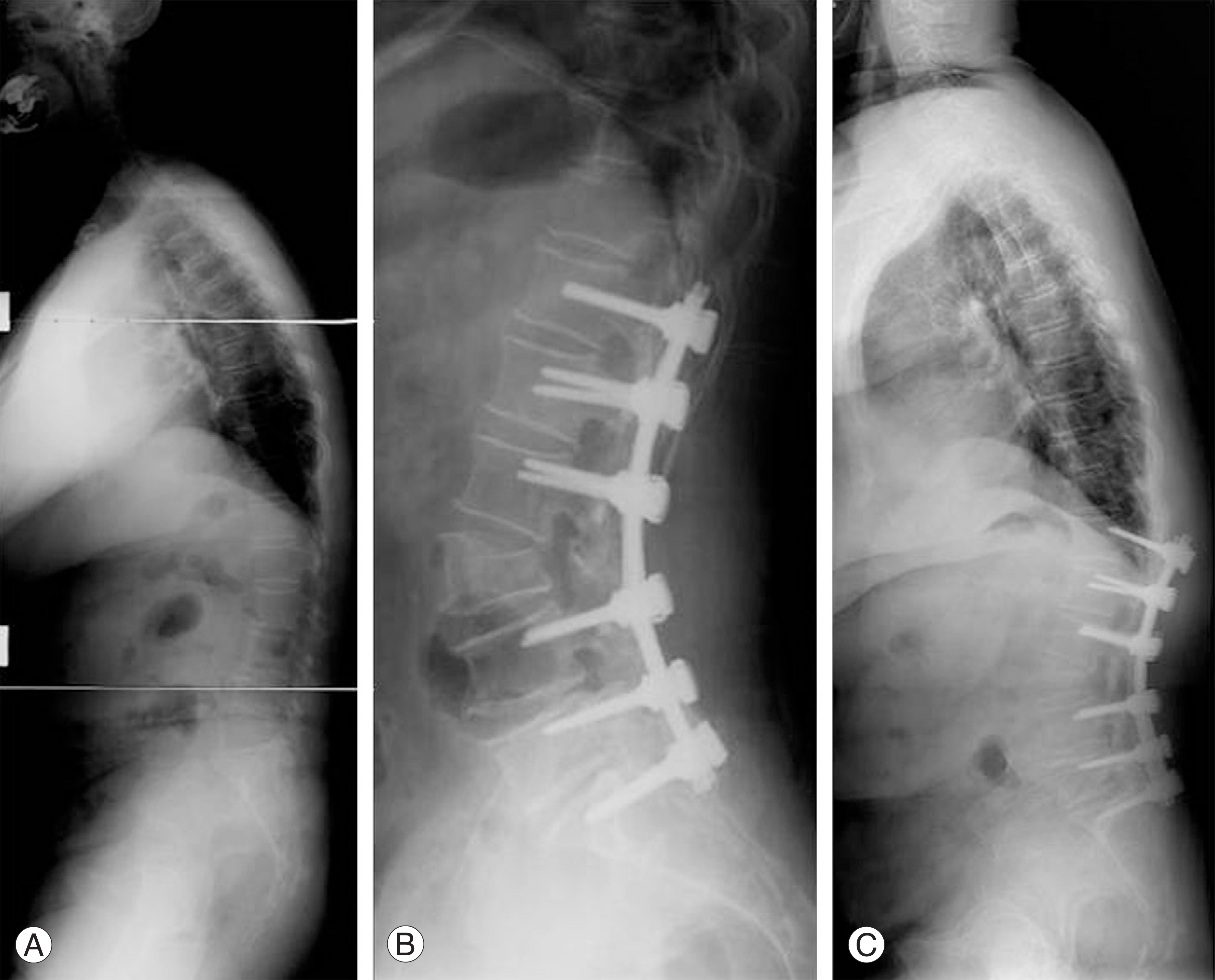
Fig. 1. A 66-year old woman with Lumbar degenerative kyphosis. (A) Preoperative thoracolumbar kyphosis 25°(B) Postoperative sagittal balance after spinal fusion from T12 to S1 and L3 PSO (C) Sagittal balance loss due to proximal screw loosening after postoperative 4 years later. PSO, Pedicle subtraction osteotomy
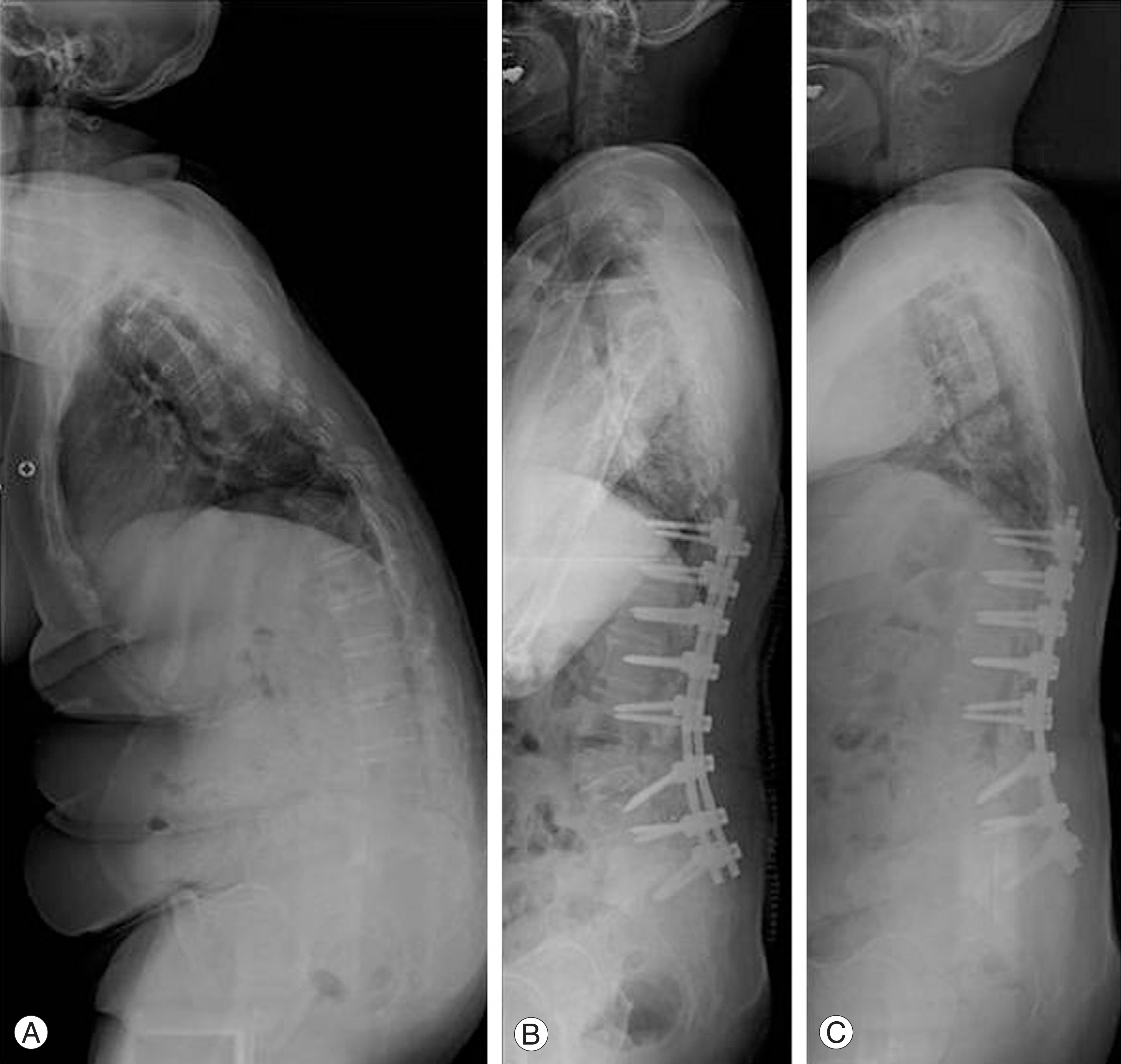
Fig. 2. A 62-year old woman with Lumbar degenerative kyphosis. (A) Preoperative thoracic kyphosis 25°, thoracolumbar kyphosis 25° (B) Proper sagittal balance after spinal fusion from T10 to S1 and L3 PSO. Postoperative lumbar lordosis -45° (C) Maintain proper sagittal balance after 2 years later operation. PSO, Pedicle subtraction osteotomy

Fig. 3. A 73-year old woman with Lumbar degenerative kyphosis. (A) Preoperative thoracic kyphosis 16°, thoracolumbar kyphosis 14°, lumbar lordosis -7°(B) Proper sagittal balance after spinal fusion from T10 to S1 with iliac screw and L3 PSO. Postoperative lumbar lordosis -45° (C) Maintain proper sagittal balance after 2 years later operation. PSO, Pedicle subtraction osteotomy
Cited by 2 articles
-
Proximal Junctional Problems in Surgical Treatment of Lumbar Degenerative Sagittal Imbalance Patients and Relevant Risk Factors
Whoan Jeang Kim, Dae Geon Song, Jae Won Lee, Jong Won Kang, Kun Young Park, Je Yun Koo, Won Cho Kwon, Won Sik Choy
J Korean Soc Spine Surg. 2013;20(4):156-162. doi: 10.4184/jkss.2013.20.4.156.Changes of Spinopelvic Parameter using Iliac Screw In Surgical Correction of Sagittal Imbalance Patients
Whoan Jeang Kim, Yong Joo Chi, Dae Geon Song, Kyung Hoon Park, Kun Young Park, Hwan Il Sung, Je Yun Koo, Won Cho Kwon, Won Sik Choy
J Korean Soc Spine Surg. 2014;21(2):63-69. doi: 10.4184/jkss.2014.21.2.63.
Reference
-
1). Lee CS, Kim YT, Kim E. Clinical Study of Lumbar Degenerative Kyphosis. J Korean Spine Surg. 1997; 4:27–35.2). Lee CS, Lee CK, Kim YT, Hong YM, Yoo JH. Dynamic Sagittal Imbalance of the Spine in Degenerative Flat Back. Spine. 2001; 26:2029–2035.
Article3). Kim HJ, Kang JW, Yeom JS, et al. .:. A Comparative Analysis of Sagittal Spinal Balance in 100 Asymptomatic Young and Older Aged Volunteers. J Korean Spine Surg. 2003; 4:327–334.
Article4). Noun Z, Lapresle P, Missenard G. Posterior lumbar osteotomy for flat back in adults. J spinal Disord. 2001; 14:311–316.
Article5). Kim HJ, Kang JW, Kim HY, et al. .:. Change of Pelvic Tilt before and after Gait in Patients with Lumbar Degenerative Kyphosis. J Korean Spine Surg. 2009; 16:95–103.
Article6). Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. An Analysis of Sagittal Spinal Alignment Following Long Adult Lumbar Instrumentation and Fusion to L5 or S1: can we predict ideal lumbar lordosis? Spine. 2006; 31:2343–2352.
Article7). Swank ML. Adjacent segment failure above lumbosacral fusions instrumented to L1 or L2. Podium presentation at the. Scoliosis Research Society;37th annual meeting. September 18-21, 2002. Seattle, WA, USA.8). Suk SI, Kim JH, Lee SM, et al. .:. Incidence of proximal adjacent failure in adult lumbar deformity correction. Podium presentation at the. Scoliosis Research Society;38th annual meeting. September 10-13, 2003. Quebec City, Canada.9). Kim YJ, Bridwell KH, Lenke LG, Rhim S, Kim YW. Is the T9, T11, or L1 the more reliable proximal level after adult lumbar or lumbosacral instrumented fusion to L5 or S1? Spine. 2007; 32:2653–2661.
Article10). Lee CS, Oh WH, Chung SS, Lee SG, Lee JY. Analysis of the Sagittal Alignment of Normal Spines. J of Korean Ortho. 1999; 34:949–954.
Article11). Bernhardt M, Bridwell KH. Segmental Analysis of the Sagittal Plane Alignment of the Normal Thoracic and Lumbar Spines and Thoracolumbar Junction. Spine. 1989; 14:717–721.
Article12). Edwards CC 2nd, Bridwell KH, Patel A, Rinella AS, Berra A, Lenke LG. Long Adult Deformity Fusions to L5 and the Sacrum A Matched Cohort Analysis. Spine. 2004; 29:1996–2005.
Article13). Bernhardr M, Swartz DE, Clothiaux PL, et al. .:. Posterolateral lumbar and lumbosacral fusion with without pedicle screw internal fixation. Clin Orthop Rela Res. 1992; 284:109–115.14). Horowitch A, Peek RD, Thomas JC Jr, et al. .:. The Wiltse pedicle screw fixation system. Early clinical results. Spine. 1989; 14:461–467.15). Molinari RW, Bridwell KH, Lenke LG, Unqacta FF, Riew KD. Complications in the surgical treatment of pediatric high-grade isthmic dysplastic spondylolisthesis. A comparison of three surgical approaches. Spine. 1999; 24:1701–1711.16). Rechtine GR, Sutterlin CE, Wood GW, Boyd RJ, Mansfield FL. The efficacy of pedicle screw/plate fixation on lumbar/lumbosacral autogenous bone graft fusion in adult patients with degenerative spondylolisthesis. J Spinal Disord. 1996; 9:382–391.
Article17). Kim HJ, Kang JW, Kim KH, et al. .:. Analysis of Correc-tiom Loss aster Pedicle subtraction Osteotomy in patients with Sagittal Imbalance? Radiologic Aspects-. J Korean Spine Surg. 2004; 39:629–635.18). Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Pseudarthrosis in long adult spinal deformity instrumentation and fusion to the sacrum: prevalence and risk factor analysis of 144 cases. Spine. 2006; 31:2329–2336.
Article19). Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C. Minimum 5-Year Analysis of L5-S1 Fusion Using Sacropelvic fixation(Bilateral S1 and Iliac screws) for Spinal Deformity. Spine. 2006; 31:303–308.20). Emami A, Deviren V, Berven S, Smith JA, Hu SS, Bradford DS. Outcome and Complications of long fusions to the Sacrum in Adult Spine Deformity: Luque-Galveston, Combined Iliac and Sacral Screws, and Sacral Fixation. Spine. 2002; 27:776–786.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Natural History of Lumbar Degenerative Kyphosis with Conservative Treatment
- Erector Spinae Atrophy Correlates with Global Sagittal Imbalance and Postoperative Proximal Junctional Kyphosis Incidence in Lumbar Degenerative Kyphosis
- Surgical Correction in Patients with Lumbar Degenerative Kyphosis Who Had Low Bone Mineral Density: An Analysis of 40 Patients with a Minimum Follow-Up of Two Years
- ‘Lumbar Degenerative Kyphosis’ Is Not Byword for Degenerative Sagittal Imbalance: Time to Replace a Misconception
- Significance of Gait Analysis in Surgical Treatment of Lumbar Degenerative Kyphosis
