Meningovascular and Spinal form of Neurosyphilis Presenting as Multiple Cranial Nerve Palsy, Cerebral Infarction and Meningomyelitis in a Human Immunodeficiency Virus Negative-Patient: MR Imaging Features
- Affiliations
-
- 1Department of Radiology, Inha University School of Medicine, Incheon, Korea. pengoon@gmail.com
- KMID: 1999927
- DOI: http://doi.org/10.13104/jksmrm.2014.18.3.263
Abstract
- Neurosyphilis is a rare infection of the brain and spinal cord caused by a spirochete named Treponema pallidum. We describe the magnetic resonance imaging of a 53-year-old man with syphilis who manifested as both meningovascular, and spinal meningomyelitic types, which involved the optic, trigeminal, facial and vestibulocochlear nerves, both middle and left posterior cerebral arteries, thoracic spinal cord and meninges of the lumbar spine. This case report suggests that neurosyphilis should be considered as a possible diagnosis in patients showing complex brain and spinal imaging features. These features include enhancing meningeal lesions with multiple cranial nerve involvement, stenoses in large to medium size cerebral arteries, and intramedullary and meningeal lesions of spine.
Keyword
MeSH Terms
-
Brain
Cerebral Arteries
Cerebral Infarction*
Constriction, Pathologic
Cranial Nerve Diseases*
Cranial Nerves
Diagnosis
HIV*
Humans
Magnetic Resonance Imaging*
Meninges
Meningitis
Middle Aged
Neurosyphilis*
Posterior Cerebral Artery
Spinal Cord
Spine
Spirochaetales
Syphilis
Tabes Dorsalis
Treponema pallidum
Vestibulocochlear Nerve
Figure
-

Fig. 1 Brain MRI of a 53-year-old man with neurosyphilis. Postcontrast axial T1-weighted images show multiple enhancements at a. The right trigeminal nerve and the Meckel's cave (arrow), b. The right facial and vestibulocochlear nerves (arrows), the right cochlea (arrow head), c, d. The optic nerves and the chiasm (short arrow). Either nodular or ring enhancing lesions are seen at basal cistern (arrow heads), left sylvian fissure (curved arrow), pituitary stalk and hypothalamus (long arrow), along with thin leptomeningeal enhancement along the basal cistern and the brain stem. e. A contrast-enhanced MRA shows a segmental stenosis at the M1 portion of the right middle cerebral artery (arrow).
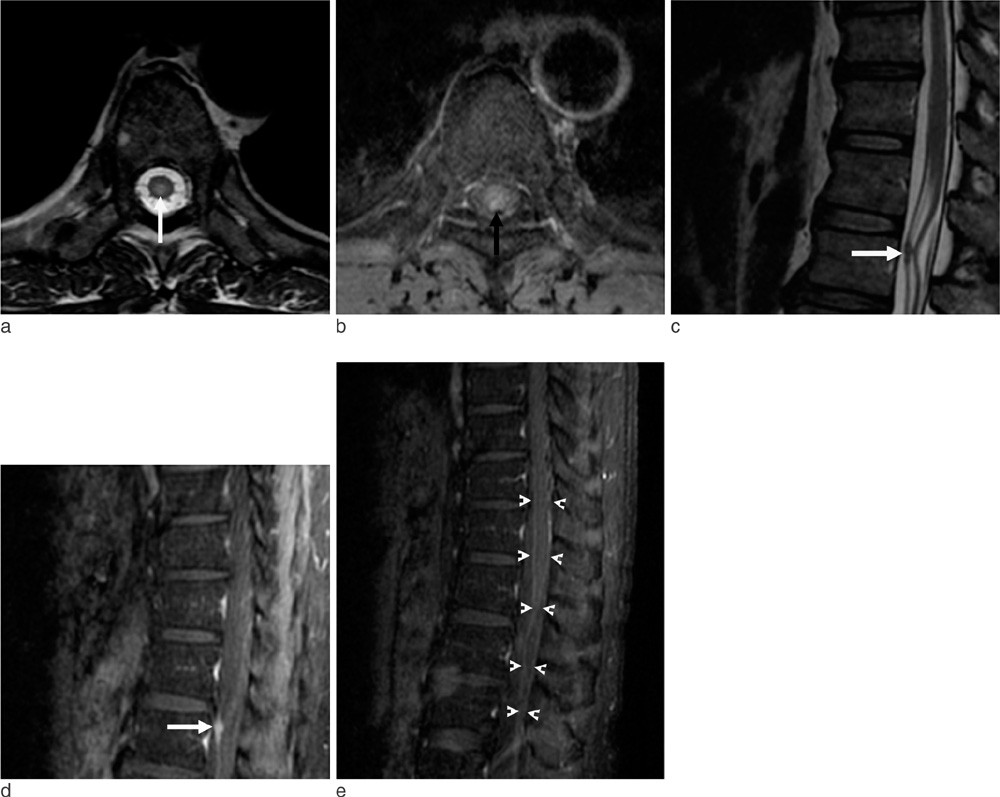
Fig. 2 Spine MRI of the patient. a. An axial T2-weighted image demonstrates a centrally located hyperintense lesion in the spinal cord at the T7 level (arrow). b. A postcontrast T1-weighted image depicts a patchy enhancing focus (arrow) in the cord that showed a T2 hyperintensity. c, d. Sagittal T2-weighted and postcontrast T1-weighted images show clumped nerve roots at the L1 level with nodular meningeal enhancement (arrows). e. A diffuse meningeal enhancement is seen along the surface of the lumbar and lower thoracic cord and the cauda equine (arrow heads).
Reference
-
1. Tien RD, Gean-Marton MD, Mark AS. Neurosyphilis in HIV carriers: MR findings in six patients. AJR Am J Roentgenol. 1992; 158:1325–1328.2. Holland BA, Perrett LV, Mills CM. Meningovascular syphilis: CT and MR findings. Radiology. 1986; 158:439–442.3. Wharton M, Chorba TL, Vogt RL, Morse DL, Buehler JW. Case definitions for public health surveillance. MMWR Recomm Resp. 1990; 39:1–43.4. Yoon YK, Kim MJ, Chae YS, Kang SH. Cerebral syphilitic gumma mimicking a brain tumor in the relapse of secondary syphilis in a human immunodeficiency virus-negative patient. J Korean Neurosurg Soc. 2013; 53:197–200.5. Chilver-Stainer L, Fischer U, Hauf M, Fux CA, Sturzenegger M. Syphilitic myelitis: rare, nonspecific, but treatable. Neurology. 2009; 72:673–675.6. Nagappa M, Sinha S, Taly AB, et al. Neurosyphilis: MRI features and their phenotypic correlation in a cohort of 35 patients from a tertiary care university hospital. Neuroradiology. 2013; 55:379–388.7. Kikuchi S, Shinpo K, Niino M, Tashiro K. Subacute syphilitic meningomyelitis with characteristic spinal MRI findings. J Neurol. 2003; 250:106–107.8. Smith MM, Anderson JC. Neurosyphilis as a cause of facial and vestibulocochlear nerve dysfunction: MR imaging features. AJNR Am J Neuroradiol. 2000; 21:1673–1675.9. Jang JH, Kim EJ, Choi WS, Yoon SS, Heo SH. Neurosyphilis involving cranial nerves in brain stem: 2 case reports. J Korean Soc Radiol. 2012; 66:11–15.10. Seeley WW, Venna N. Neurosyphilis presenting with gummatous oculomotor nerve palsy. J Neurol Neurosurg Psychiatry. 2004; 75:789.11. Ghanem KG. Review: Neurosyphilis: A historical perspective and review. CNS Neurosci Ther. 2010; 16:e157–e168.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Neurosyphilis with Acute Optic Neuritis and Trochlear Nerve Palsy in Human Immunodeficiency Virus Infected Male
- Neurosyphilis Involving Cranial Nerves in Brain Stem: 2 Case Reports
- Cryptococcal Meningoencephalitis Presenting as Cerebral Infarction and Multiple Cranial Nerve Palsies
- Cerebral Gumma Mimicking a Brain Tumor in a Human Immunodeficiency Virus-Negative Patient: A Case Report
- Combined Facial and Contralateral Trochlear Nerve Palsy in a Patient with Diabetes Mellitus
