The Secondary Contiguous or Non-contiguous Subchondral Bone Impactions in Subaxial Cervical Spinal Injury: Incidence and Associated Primary Injury Patterns
- Affiliations
-
- 1Department of Radiology, Inha University Hospital, Incheon, Korea. kimyeoju@hanmail.net
- 2Department of Neurosurgery, Inha University Hospital, Incheon, Korea.
- 3Department of Orthopedics, Inha University Hospital, Incheon, Korea.
- KMID: 1999923
- DOI: http://doi.org/10.13104/jksmrm.2014.18.3.232
Abstract
- PURPOSE
To evaluate the incidence of secondary contiguous or non-contiguous subchondral bone impactions (SBI) in subaxial cervical spinal injury and associated primary injury patterns.
MATERIALS AND METHODS
A retrospective review of computed tomography, magnetic resonance imaging, and medical records was carried out for 47 patients who had sustained a subaxial cervical spinal injury. Presence, number, level, and sites of secondary contiguous or non-contiguous SBI were recorded. To evaluate primary injury patterns, the level and number of primary injury sites of subaxial cervical spine injury, injury morphology, anterior/posterior discoligamentous complex (ADC/PDC) injury, posterior ligamentous complex (PLC) injury, spinal cord injury, and mechanism of injury (MOI) were analyzed. Differences in primary injury pattern of subaxial cervical spine injury and MOI between patients with and without SBI, and between contiguous or non-contiguous SBI were analyzed using the Mann-Whitney U test, Pearson's chi square test and Fisher's exact test.
RESULTS
Eighteen patients (18/47, 38.29%) had developed contiguous (n=9) or non-contiguous (n=9) SBI, most commonly involving T3 (15/47, 31.91%) and 3 levels (6/18, 33.33%). All SBIs had developed near the anterosuperior region of the body and the superior endplate and were the result of a high-impact MOI. SBIs were statistically significant in association with injury morphology and PLC injury (P=0.001, P=0.009, respectively) at the primary injury site. Non-contiguous SBI was more frequently accompanied by upper cervical spinal injuries in association with PDC injuries, as opposed to contiguous SBI, with statistical significance (P=0.009), while no other statistically significant differences were found.
CONCLUSION
Secondary SBIs are common and probably associated with subaxial cervical spinal injuries with high energy compressive flexion forces.
Keyword
MeSH Terms
Figure
-
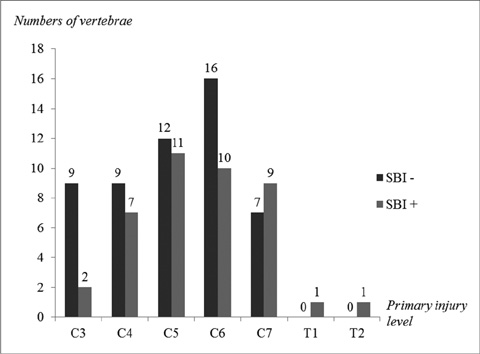
Fig. 1 A graph of the number of the primary injury level in patients with (+) and without (-) SBI.

Fig. 2 A graph of the number of vertebrae according to the level of contiguous and non-contiguous secondary SBI.
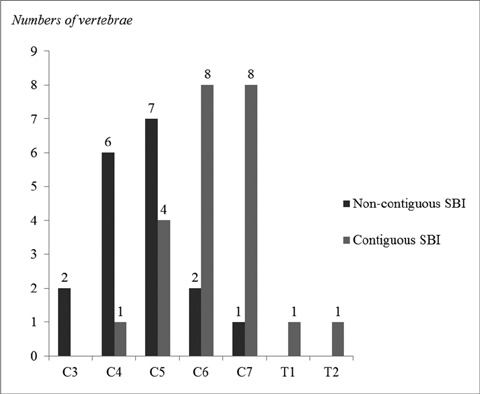
Fig. 3 A graph of the number of the primary injury level in patients with contiguous and non-contiguous SBI.

Fig. 4 Images of a 36-year-old man with non-contiguous SBIs in a subaxial cervical spinal injury. Saggital CT images (a, b) show anterior translation of C4 on C5 with right unilateral facet locking with fractures, representing translation morphology according to the SLIC system. Sagittal STIR (c) and contrast enhanced T1-weighted MR images with fat suppression (d), showing non-contiguous SBIs at the vertebral body near the superior endplates from C7 to T3 (arrows). High signal intensity is noted at the interspinous area of C1-2 and C4-5 level (white arrowheads in c), suggesting posterior ligamentous complex injury. There is also irregularly high signal intensity at the posterior portion of the disc, with herniation at the C4-5 level (black arrowhead in c), representing posterior discoligamentous complex injury.
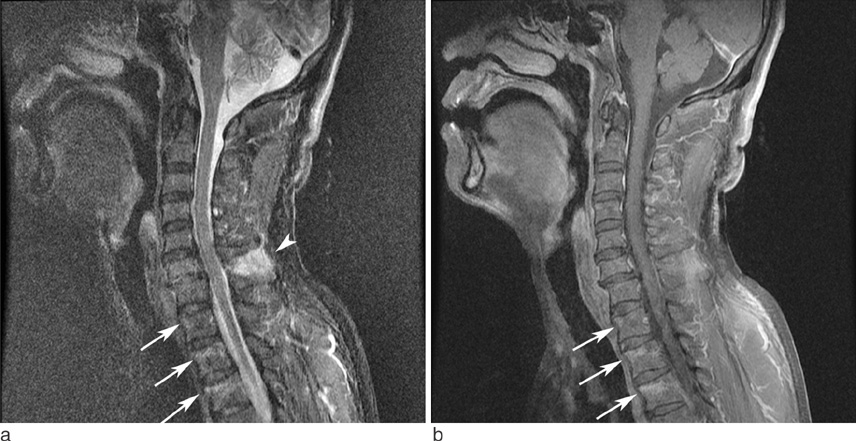
Fig. 5 Images of a 58-year-old man with contiguous SBIs in subaxial cervical spinal injury. STIR (a) and sagittal contrast enhanced T1-weighted MR images with fat suppression (b) show mild anterior translation of the C6 vertebral body on C7, representing translation morphology. Contiguous SBIs are seen near the superior endplates from the T1 to the T3 level (arrows in a, b). High signal intensity is noted at the interspinous area of the C6-7 level (arrowhead in a), representing posterior ligamentous complex injury.
Reference
-
1. Griffith HB, Gleave JR, Taylor RG. Changing patterns of fracture in the dorsal and lumbar spine. Br Med J. 1966; 1:891–894.2. Bentley G, McSweeney T. Multiple spinal injuries. Br J Surg. 1968; 55:565–570.3. Kewalramani LS, Taylor RG. Multiple non-contiguous injuries to the spine. Acta Orthop Scand. 1976; 47:52–58.4. Calenoff L, Chessare JW, Rogers LF, Toerge J, Rosen JS. Multiple level spinal injuries: importance of early recognition. AJR Am J Roentgenol. 1978; 130:665–669.5. Korres DS, Katsaros A, Pantazopoulos T, Hartofilakidis-Garofalidis G. Double or multiple level fractures of the spine. Injury. 1981; 13:147–152.6. Tearse DS, Keene JS, Drummond DS. Management of non-contiguous vertebral fractures. Paraplegia. 1987; 25:100–105.7. Gupta A, el Masri WS. Multilevel spinal injuries. Incidence, distribution and neurological patterns. J Bone Joint Surg Br. 1989; 71:692–695.8. Keenen TL, Antony J, Benson DR. Non-contiguous spinal fractures. J Trauma. 1990; 30(4):489–491. Epub 1990/04/01.9. Henderson RL, Reid DC, Saboe LA. Multiple noncontiguous spine fractures. Spine (Phila Pa 1976). 1991; 16:128–131.10. Vaccaro AR, An HS, Lin S, Sun S, Balderston RA, Cotler JM. Noncontiguous injuries of the spine. J Spinal Disord. 1992; 5:320–329.11. Green RA, Saifuddin A. Whole spine MRI in the assessment of acute vertebral body trauma. Skeletal Radiol. 2004; 33:129–135.12. Qaiyum M, Tyrrell PN, McCall IW, Cassar-Pullicino VN. MRI detection of unsuspected vertebral injury in acute spinal trauma: incidence and significance. Skeletal Radiol. 2001; 30:299–304.13. Eustace S, Keogh C, Blake M, Ward RJ, Oder PD, Dimasi M. MR imaging of bone oedema: mechanisms and interpretation. Clinical Radiology. 2001; 56:4–12.14. Teli M, de Roeck N, Horwitz MD, Saifuddin A, Green R, Noordeen H. Radiographic outcome of vertebral bone bruise associated with fracture of the thoracic and lumbar spine in adults. Eur Spine J. 2005; 14:541–545.15. Sanders TG, Medynski MA, Feller JF, Lawhorn KW. Bone contusion patterns of the knee at MR imaging: footprint of the mechanism of injury. Radiographics. 2000; 20:S135–S151.16. Sijbrandij ES, van Gils AP, Louwerens JW, de Lange EE. Posttraumatic subchondral bone contusions and fractures of the talotibial joint: occurrence of "kissing" lesions. AJR Am J Roentgenol. 2000; 175:1707–1710.17. Vaccaro AR, Hulbert RJ, Patel AA, et al. The subaxial cervical spine injury classification system: a novel approach to recognize the importance of morphology, neurology, and integrity of the disco-ligamentous complex. Spine (Phila Pa 1976). 2007; 32:2365–2374.18. Aarabi B, Walters BC, Dhall SS, et al. Subaxial cervical spine injury classification systems. Neurosurgery. 2013; 72:170–186.19. Goradia D, Linnau KF, Cohen WA, Mirza S, Hallam DK, Blackmore CC. Correlation of MR imaging findings with intraoperative findings after cervical spine trauma. AJNR Am J Neuroradiol. 2007; 28:209–215.20. Demaerel P. Magnetic resonance imaging of spinal cord trauma: a pictorial essay. Neuroradiology. 2006; 48:223–232.21. Bohndorf K. Imaging of acute injuries of the articular surfaces (chondral, osteochondral and subchondral fractures). Skeletal Radiol. 1999; 28:545–560.22. Delgado Almandoz JE, Schaefer PW, Kelly HR, Lev MH, Gonzalez RG, Romero JM. Multidetector CT angiography in the evaluation of acute blunt head and neck trauma: a proposed acute craniocervical trauma scoring system. Radiology. 2010; 254:236–244.23. Choi SJ, Shin MJ, Kim SM, Bae SJ. Non-contiguous spinal injury in cervical spinal trauma: evaluation with cervical spine MRI. Korean J Radiol. 2004; 5:219–224.24. Panjabi MM, White AA 3rd. Basic biomechanics of the spine. Neurosurgery. 1980; 7:76–93.25. Allen BL Jr, Ferguson RL, Lehmann TR, O'Brien RP. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine (Phila Pa 1976). 1982; 7:1–27.26. Rihn JA, Fisher C, Harrop J, Morrison W, Yang N, Vaccaro AR. Assessment of the posterior ligamentous complex following acute cervical spine trauma. J Bone Joint Surg Am. 2010; 92:583–589.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Non-Contiguous Spinal Injury in Cervical Spinal Trauma: Evaluation with Cervical Spine MRI
- Multiple Non-contiguous Spine Fractures with Concomitant Injuries: A Case Report
- Non - Contiguous Multiple Spine Fracture
- Kinematical Characteristics of the Translational and Pendular Movements of each Cervical Vertebra at the Flexion and Extension Motion
- Treatment of Cervical Cord Injury with Ankylosing Spondylitis: Case Report
