Clinical evaluation of a new extraction method for intentional replantation
- Affiliations
-
- 1Department of Conservative Dentistry, Section of Dentistry, Seoul National University Bundang Hospital, Seongnam, Korea. yhchoi@snubh.org
- KMID: 1986685
- DOI: http://doi.org/10.5395/JKACD.2011.36.3.211
Abstract
- PURPOSE
Intentional replantation (IR) is a suitable treatment option when nonsurgical retreatment and periradicular surgery are unfeasible. For successful IR, fracture-free safe extraction is crucial step. Recently, a new extraction method of atraumatic safe extraction (ASE) for IR has been introduced.
PATIENTS AND METHODS
Ninety-six patients with the following conditions who underwent IR at the Department of Conservative Dentistry, Seoul National University Bundang Hospital, in 2010 were enrolled in this study: failed nonsurgical retreatment and periradicular surgery not recommended because of anatomical limitations or when rejected by the patient. Preoperative orthodontic extrusive force was applied for 2-3 weeks to increase mobility and periodontal ligament volume. A Physics Forceps was used for extraction and the success rate of ASE was assessed.
RESULTS
Ninety-six premolars and molars were treated by IR. The complete success rate (no crown and root fracture) was 93% (n = 89); the limited success rates because of partial root tip fracture and partial osteotomy were 2% (n = 2) and 5% (n = 5), respectively. The clinical and overall success rates of ASE were 95% and 100%, respectively; no failure was observed.
CONCLUSIONS
ASE can be regarded as a reproducible, predictable method of extraction for IR.
Keyword
MeSH Terms
Figure
-
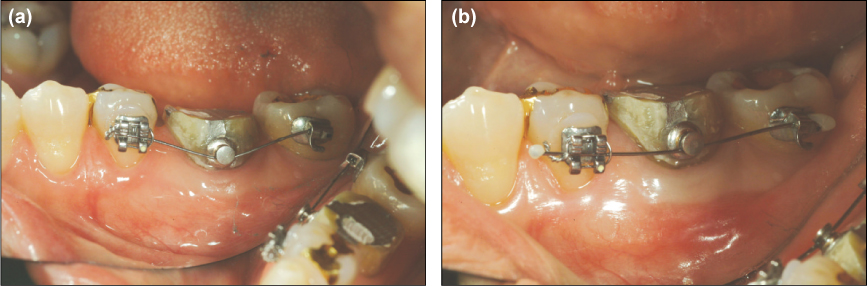
Figure 1 (a) Orthodontic brackets and wire attached to a left mandibular first molar requiring IR. In this case, a button was used; however, any devices can be used as long as an extrusive force is applied. (b) Twenty-two days after orthodontic extrusive force was applied. Given the straightening of the wire, tooth extrusion was assumed to have occurred; concurrently, mobility increased.

Figure 2 (a) Extrusive force was applied on the most posterior tooth, using a .016 × .022 TMA wire as a coil spring. (b) If no appropriate anchor position is available, an orthodontic implant can be used for anchorage.

Figure 3 (a) Positioning of the Physics Forceps. Ensure that the beak is placed only on the lingual root surface to significantly reduce the possibility of crown or root fracture. (b) Extraction procedure. A weak but consistent force was applied for extraction. The mandibular left 1st molar was extracted with rotational force. (c) Once the tooth rotated, then conventional forcep was used to extracted completely. The extraction time in this case was 1 minute 17 seconds. (photograph of another patient)

Figure 4 (a) The maxillary first molar was successfully extracted by ASE. The extraction time was 5 minutes 17 seconds. (b) Limited success with root tip fracture. The curved distolingual root tip of the mandibular left molar fractured during extraction. The extraction time was 4 minutes. (c) Limited success with osteotomy. The maxillary first molar showed no increased mobility after orthodontic extrusion; its divergent buccal and palatal roots and particularly thick buccal cortical bone were possibly responsible. The extraction time including osteotomy was 10 minutes 31 seconds.

Figure 5 The mandibular second molar was extracted concurrently with the septal bone. The extraction time was 15 minutes 46 seconds.
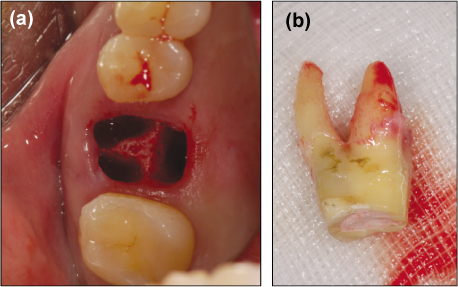
Figure 6 (a) Extraction socket of a right maxillary first molar. No soft tissue damage is observable, and the alveolar bone is well preserved. (b) The extracted tooth. The extraction time was 3 minutes 30 seconds.

Figure 7 An extracted right maxillary second premolar. The elongated periodontal ligament attached to the root area can be seen, helping the replanted tooth to heal uneventfully.

Figure 8 A maxillary premolar extracted for orthodontic treatment. The beak of the forceps is located in the subgingival area, damaging the periodontal ligament, gingiva, and alveolar bone. The greater is the damage to the marginal tissue, the less likely is primary closure.
Cited by 1 articles
-
Surgical extrusion of a maxillary premolar after orthodontic extrusion: a retrospective study
Yong-Hoon Choi, Hyo-Jung Lee
J Korean Assoc Oral Maxillofac Surg. 2019;45(5):254-259. doi: 10.5125/jkaoms.2019.45.5.254.
Reference
-
1. Grossman LI. Intentional replantation of teeth: a clinical evaluation. J Am Dent Assoc. 1982. 104:633–639.
Article2. Kingsbury BC Jr, Wiesenbaugh JM Jr. Intentional replantation of mandibular premolars and molars. J Am Dent Assoc. 1971. 83:1053–1057.
Article3. Benenati FW. Intentional replantation of a mandibular second molar with long-term follow-up: report of a case. Dent Traumatol. 2003. 19:233–236.
Article4. Peer M. Intentional replantation - a 'last resort' treatment or a conventional treatment procedure? nine case reports. Dent Traumatol. 2004. 20:48–55.
Article5. Kratchman S. Intentional replantation. Dent Clin North Am. 1997. 41:603–617.6. Bender IB, Rossman LE. Intentional replantation of endodontically treated teeth. Oral Surg Oral Med Oral Pathol. 1993. 76:623–630.
Article7. Assif D, Gorfil C. Biomechanical considerations in restoring endodontically treated teeth. J Prosthet Dent. 1994. 71:565–567.
Article8. Al-Shammari KF, Kazor CE, Wang HL. Molar root anatomy and management of furcation defects. J Clin Periodontol. 2001. 28:730–740.
Article9. Misch CE, Perez HM. Atraumatic extractions: a biomechanical rationale. Dent Today. 2008. 27:98100–101.10. Choi YH, Bae JH, Kim YK. Atraumatic safe extraction for intentional replantation. J Korean Dent Assoc. 2010. 48:531–537.11. Sorensen JA, Engelman MJ. Ferrule design and fracture resistance of endodontically treated teeth. J Prosthet Dent. 1990. 63:529–536.
Article12. Hayashi H. Ortho-transplantation. 2006. 1st ed. Seoul: Narae Publishing Co.;18–28.13. Tsukiboshi M, Andreasen J, Asai Y. Autotransplantation of teeth. 2001. 1st ed. Tokyo: Quintessence;22–40.14. Kany FM. Single-tooth osteotomy for intention replantation. J Endod. 2002. 28:408–410.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intentional replantation with preapplication of orthodontic force on mandibular second molar
- Treatment of a tooth with severe periodontal involvement using intentional replantation: case report
- Short-term clinical outcome of intentionally replanted posterior molars
- Changes in periodontium after extraction of a periodontally-involved tooth in rats
- Surgical management with intentional replantation on a tooth with palato-radicular groove
