Short-term clinical outcome of intentionally replanted posterior molars
- Affiliations
-
- 1Department of Conservative Dentistry, Section of Dentistry Seoul National University Bundang Hospital, Seongnam, Korea. yhchoi@snubh.org
- KMID: 1446079
- DOI: http://doi.org/10.5395/JKACD.2011.36.1.12
Abstract
OBJECTIVES
This retrospective study evaluated the therapeutic effects of the intentional replantation (IR) procedure performed on the maxillary and mandibular molars of 35 patients.
MATERIALS AND METHODS
For the subjects, IR was performed due to difficulties in anatomically accessing the lesions and/or close proximity to the thick cortical bone, inferior alveolar nerve, or maxillary sinus, which rendered the ordinary periradicular surgery impossible. The patients' progress was followed for a year and up to 2 years and 4 months. The success of the procedure was evaluated in terms of clinical and radiographic success (%).
RESULTS
The results revealed the following: (a) 1 case (3%) of failed tooth extraction during IR; (b) 2 cases (6%) of extraction due to periodontal diseases and inflammatory root resorption; (c) 3 cases (9%) of normally functioning teeth in the oral cavity with minor mobility and apical root resorption, and; (d) 29 cases (82%) of normally functioning teeth without obvious problems.
CONCLUSIONS
IR was confirmed to be a reliably repeatable, predictable treatment option for those who cannot receive conventional periradicular surgery because of anatomic limitations or patient factors.
MeSH Terms
Figure
-
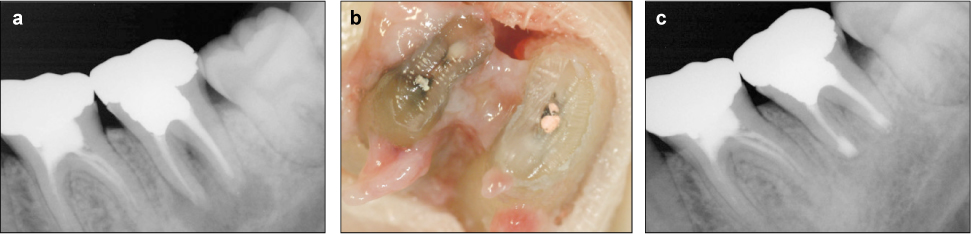
Figure 1 (a) Periapical radiograph of a second mandibular molar with a large periapical lesion. Patient (28-year-male) refused non-surgical retreatment and just wanted simple extraction of second molar then implant therapy. (b) Extracted mandibular second molar. Apical 3 mm was resected using diamond high speed bur. Calcification was observed in the mesiobuccal canal connected with mesiolingual canal via an isthmus. Retrograde filling was performed using MTA. Extracting the tooth took 1 minute and 23 seconds, with the extra oral root end treatment taking 9 minutes and 56 seconds. (c) 1.5 years after intentional replantation, the radiograph shows complete healing and no evidence of external root resorption.

Figure 2 (a) Periapical radiograph of a first mandibular molar showing brocken root canal instrument and long canal post. (b) GP cone tracing through buccal fistula showed the origin was periapical lesion of the first mandibular molar. Non-surgical retreatment was the first choice of treatment but failed to remove or bypass the brocken instrument. Intentional replantation was indicated because of accessibility to the disto-lingual canal and thick buccal cortical bone. Extraction time was 58 seconds and extra-alveolar time was 14 minutes and 40 seconds. (c) 1 year after intentional replantation: The buccal fistula disappeared. No mobility of the tooth or formation of the periodontal pocket was observed. 80 days after the procedure, preliminary resin build up was performed to ensure the tooth's contact with opposing teeth. After clinical and radiological examinations confirmed the absence of problems, permanent cast gold crown was cemented 112 days after the procedure.
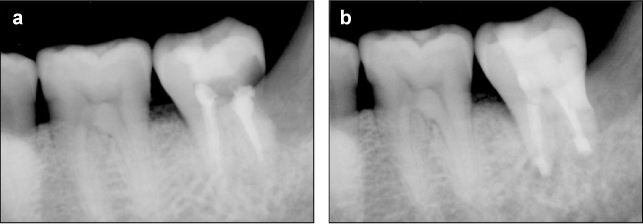
Figure 3 (a) The mandibular second molar treated for deep subgingival caries on the distal root surface: Despite the endodontic therapy provided, the patient complained of discomfort during mastication. The leakage in the distal end was not resolved, either. Thus, root end treatment and distal decay treatment were decided via intentional replantation. (b) 1 year after intentional replantation: The molar was mobile, showing unsatisfactory healing. Nonetheless, it was still functional, causing no obvious problems. Periodontal pockets were not observed, although mobility was found to have increased slightly; root absorption was detected.
Reference
-
1. Grossman LI. Intentional replantation of teeth: a clinical evaluation. J Am Dent Assoc. 1982. 104(5):633–639.
Article2. Dryden JA, Arens DE. Intentional replantation. A viable alternative for selected cases. Dent Clin North Am. 1994. 38(2):325–353.3. Weine FS. The case against intentional replantation. J Am Dent Assoc. 1980. 100(5):664–668.
Article4. Friedman S, Mor C. The success of endodontic therapy-healing and functionality. J Calif Dent Assoc. 2004. 32(6):493–503.5. Jin GC, Kim KD, Roh BD, Lee CY, Lee SJ. Buccal bone plate thickness of the Asian people. J Endod. 2005. 31(6):430–434.
Article6. Cohen S, Hargreaves KM. Pathways of the pulp. 2006. 9th ed. St. Louis, MO.;London: Elsevier Mosby;767.7. Penarrocha M, Garcia B, Marti E, Palop M, von Arx T. Intentional replantation for the management of maxillary sinusitis. Int Endod J. 2007. 40(11):891–899.
Article8. Bender IB, Rossman LE. Intentional replantation of endodontically treated teeth. Oral Surg Oral Med Oral Pathol. 1993. 76(5):623–630.
Article9. Nosonowitz DM, Stanley HR. Intentional replantation to prevent predictable endodontic failures. Oral Surg Oral Med Oral Pathol. 1984. 57(4):423–432.
Article10. Guy SC, Goerig AC. Intentional replantation: technique and rationale. Quintessence Int Dent Dig. 1984. 15(6):595–603.11. Friedman S, Lustmann J, Shaharabany V. Treatment results of apical surgery in premolar and molar teeth. J Endod. 1991. 17(1):30–33.
Article12. Hepworth MJ, Friedman S. Treatment outcome of surgical and non-surgical management of endodontic failures. J Can Dent Assoc. 1997. 63(5):364–371.13. Kingsbury B Jr, Wiesenbaugh J Jr. Intentional replantation of mandibular premolars and molars. The Journal of the American Dental Association. 1971. 83(5):1053.
Article14. Koenig KH, Nguyen NT, Barkhordar RA. Intentional replantation: a report of 192 cases. Gen Dent. 1988. 36(4):327–331.15. Barnett RJ, Burton WE, Nuckles DB. Intentional replantation: report of a successful case. Quintessence Int. 1992. 23(11):755–757.16. Raghoebar GM, Vissink A. Results of intentional replantation of molars. J Oral Maxillofac Surg. 1999. 57(3):240–244.
Article17. Peer M. Intentional replantation - a 'last resort' treatment or a conventional treatment procedure? nine case reports. Dent Traumatol. 2004. 20(1):48–55.
Article18. Lee YM, Park JW, Kim SK. Intentional replantation: An alternative treatment option when root canal treatment failed. 2003. In : Spring Scientific Meeting of Korean Academy of Conservative Dentistry; 286–287.19. Kim WC, Yoo MK, LEE KW. Treatment of congenitally abnormal tooth using intentional replantation. 2004. In : Spring Scientific Meeting of Korean Academy of Conservative Dentistry; 320–321.20. Moon JD, Heo B. Intentional replantation: A case report. 2004. In : Spring Scientific Meeting of Korean Academy of Conservative Dentistry; 322–325.21. Hayashi M, Kinomoto Y, Miura M, Sato I, Takeshige F, Ebisu S. Short-term evaluation of intentional replantation of vertically fractured roots reconstructed with dentin-bonded resin. J Endod. 2002. 28(2):120–124.
Article22. Messkoub M. Intentional replantation: a successful alternative for hopeless teeth. Oral Surg Oral Med Oral Pathol. 1991. 71(6):743–747.
Article23. Andreasen JO, Hjorting-Hansen E. Replantation of teeth. I. Radiographic and clinical study of 110 human teeth replanted after accidental loss. Acta Odontol Scand. 1966. 24(3):263–286.
Article24. Kratchman S. Intentional replantation. Dent Clin North Am. 1997. 41(3):603–617.25. Andreasen J, Hjørting-Hansen E. Replantation of teeth. II. Histological study of 22 replanted anterior teeth in humans. Acta Odontologica Scandinavica. 1966. 24(3):287–306.
Article26. Choi YH, Bae JH, Kim YK. Atraumatic safe extraction for intentional replantation. J Korean Dent Assoc. 2010. 48(7):531–537.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A retrospective study of the intentionally replanted mandibular second molars with C-shaped root canal configurations
- Evaluation of the periodontal and pulpal healing of replanted rat molars with doxycycline root conditioning
- The second molars in orthodontics
- Prognosis and Prognostic Factors of Caudate Hemorrhage
- Type I Chiari Malformation Without Concomitant Bony Instability: Assessment of Different Surgical Procedures and Outcomes in 73 Patients
