Cardiac Involvement in Hypereosinophilia Associated with Toxocariasis
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea. kyoungim74@gmail.com
- KMID: 1980428
- DOI: http://doi.org/10.4250/jcu.2014.22.4.224
Abstract
- Cardiac involvement in hypereosinophilia is rare; when present, it manifests as ventricular thickening, usually with fibrous tissue and mural thrombosis. We present a case of a 57-year-old man with an abnormal right ventricular apex with eosinophilia, which was caused by Toxocara canis infection.
Keyword
Figure
-
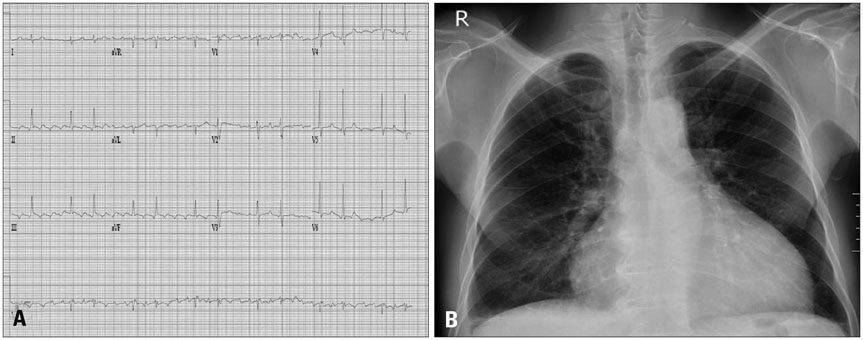
Fig. 1 Electrocardiography demonstrated atrial flutter with a ventricular rate of 77 bpm (A). Chest radiograph showed cardiomegaly and blunting of the bilateral costophrenic angles (B).
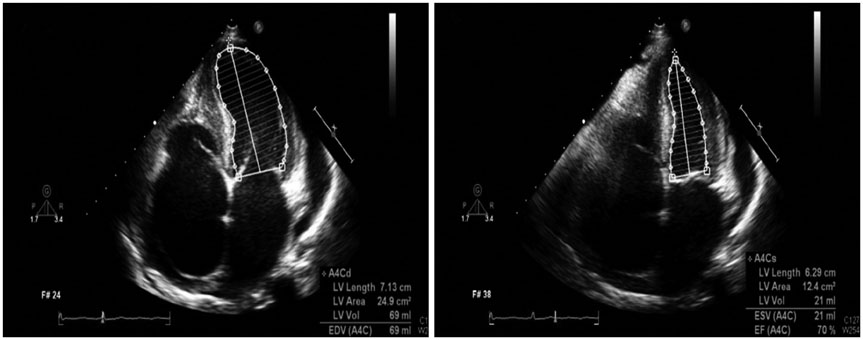
Fig. 2 Transthoracic echocardiography showed an enlarged right atrium with spontaneous echo contrast without a definite thrombus and a normal left ventricular ejection fraction.
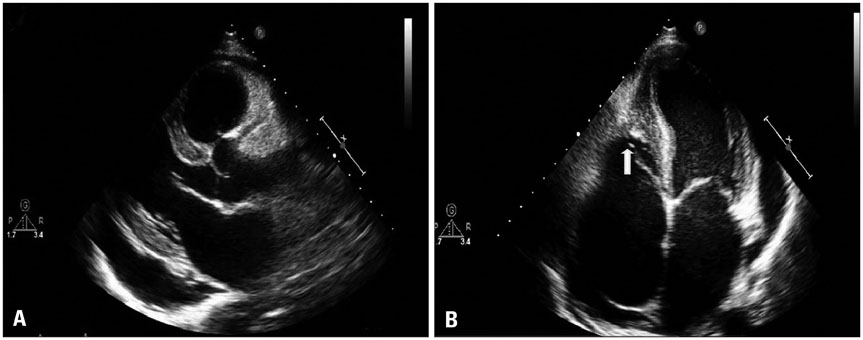
Fig. 3 There was a moderate pericardial effusion (A) and dense right ventricular apical trabeculations with a large hypoechogenic mass (arrow) occupying the apex (B).
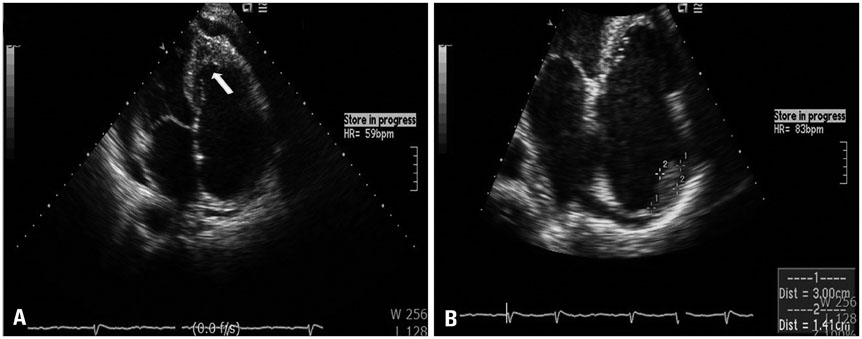
Fig. 4 Right ventricular apical trabeculations with a hypoechogenic mass (arrow) occupying the apex existed 3 months prior at the outside hospital (A). A right atrial thrombus existed at that time (B), which disappeared after anticoagulation.
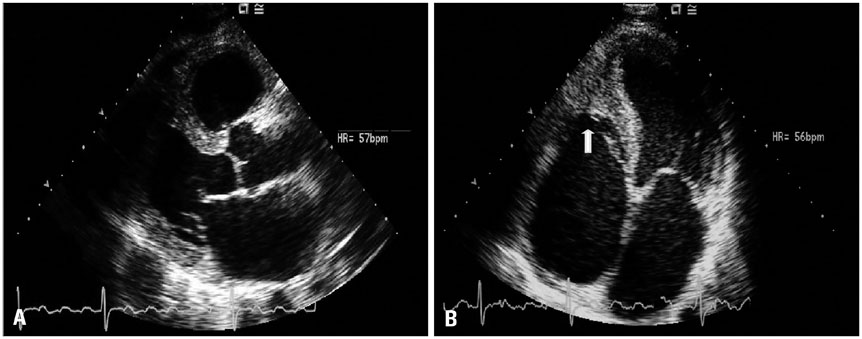
Fig. 5 After pericardiostomy, the pericardial effusion disappeared (A), and the dense right ventricular apical mass (arrow) was not altered (B).
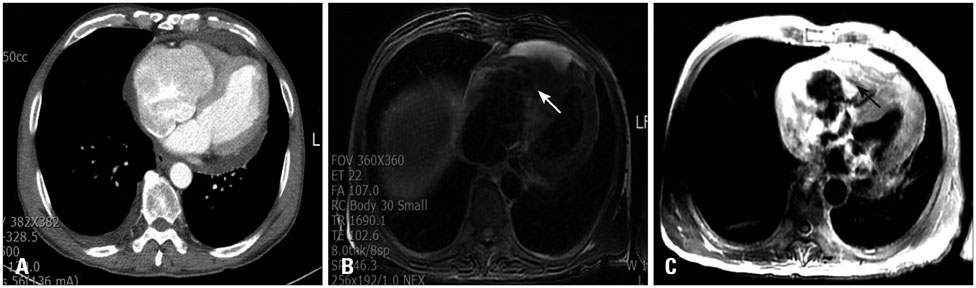
Fig. 6 Chest computerized tomography showed a relatively hypodense, thickened right ventricular apical endomyocardium (A). Cardiac magnetic resonance imaging showed a thickened, hypodense right ventricular apex (white arrow, B) and hyperenhancement of the endomyocardial border (black arrow) was shown after administration of gadolinium (C).
Reference
-
1. Tefferi A, Patnaik MM, Pardanani A. Eosinophilia: secondary, clonal and idiopathic. Br J Haematol. 2006; 133:468–492.
Article2. Kleinfeldt T, Nienaber CA, Kische S, Akin I, Turan RG, Körber T, Schneider H, Ince H. Cardiac manifestation of the hypereosinophilic syndrome: new insights. Clin Res Cardiol. 2010; 99:419–427.
Article3. Despommier D. Toxocariasis: clinical aspects, epidemiology, medical ecology, and molecular aspects. Clin Microbiol Rev. 2003; 16:265–272.
Article4. Salanitri GC. Endomyocardial fibrosis and intracardiac thrombus occurring in idiopathic hypereosinophilic syndrome. AJR Am J Roentgenol. 2005; 184:1432–1433.
Article5. Parrillo JE. Heart disease and the eosinophil. N Engl J Med. 1990; 323:1560–1561.
Article6. Sheikh J, Weller PF. Clinical overview of hypereosinophilic syndromes. Immunol Allergy Clin North Am. 2007; 27:333–355.
Article7. Lofiego C, Ferlito M, Rocchi G, Biagini E, Perugini E, Branzi A, Rapezzi C. Ventricular remodeling in Loeffler endocarditis: implications for therapeutic decision making. Eur J Heart Fail. 2005; 7:1023–1026.
Article8. Alter P, Maisch B. Endomyocardial fibrosis in Churg-Strauss syndrome assessed by cardiac magnetic resonance imaging. Int J Cardiol. 2006; 108:112–113.
Article9. Prunier F, Delépine S, Victor J, de Gentile L, Moreau C, Laporte J, Dupuis JM, Geslin P. [Loffler's fibroblastic endocarditis. A report of a case complicating toxocarosis]. Arch Mal Coeur Vaiss. 2001; 94:226–230.10. Herry I, Philippe B, Hennequin C, Danel C, Lejeunne C, Meyer G. Acute life-threatening toxocaral tamponade. Chest. 1997; 112:1692–1693.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reversible Encephalopathy Caused by Reactive Hypereosinophilia due to Toxocariasis
- A Rare Cause of Peripheral Vascular Thrombosis: Hypereosinophilia Caused by Toxocara canis Infection
- Eosinophilic Myocarditis-Associated Toxocariasis
- Transient global amnesia associated with toxocariasis and secondary hypereosinophilia
- Cerebral Toxocariasis Presented With Seizure and Memory Disturbance
