Incidentally Detected Situs Ambiguous in Adults
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, School of Medicine, The Catholic University of Korea, Seoul, Korea. younhj@catholic.ac.kr
- KMID: 1980386
- DOI: http://doi.org/10.4250/jcu.2011.19.4.211
Abstract
- Situs ambiguous is rare congenital anomaly in adults. In 2 adult patients who admitted for different cardiac problems, situs ambiguous with polysplenia was detected. A 42-year-old male admitted for radio frequent catheter ablation of atrial fibrillation, and he had left-sided inferior vena cava (IVC), hepatic segment of IVC interruption with hemiazygos continuation, multiple spleens and intestinal malrotation. And in a 52-year-old female case who was hospitalized due to infective endocarditis after implanting pacemaker for sick sinus syndrome, multiple spleens, left-sided stomach, bilateral liver with midline gallbladder, and left-sided IVC were found. Those findings were consistent with situs ambiguous with polysplenia, but their features were distinctive.
Keyword
MeSH Terms
Figure
-

Fig. 1 Double the shadow of thoracic aorta (bold arrows) and widening state of superior mediastinum (sharp arrows) were shown in chest X-ray.

Fig. 2 (A) Coronary multidirectional computed tomography: There was an 1.7 cm sized, round, tubular structure which was paralleling with descending thoracic aorta (white arrows). (B-D) On abdomen computed tomography: (B) A dilated hemiazygos vein runs posterior to the descending aorta. (C) Multiple, well-defined round soft tissue densities were detected around the spleen (black stars). IVC was located at the left side of aorta, and hepatic segment of IVC was absent. (D) Left-sided colon (hollow arrow) and right-sided small bowels (bold arrow) indicated gastrointestinal malrotation. IVC: inferior vena cava.

Fig. 3 Venography of IVC through right femoral vein: Interruption of the thoracic IVC with hemiazygos continuation (arrows) along with aortic arch was confirmed. Enlarged hemiazygos vein drained into left brachiocephalic vein and then to superior vena cava. Infra-hepatic segment of IVC was intact. IVC: inferior vena cava.
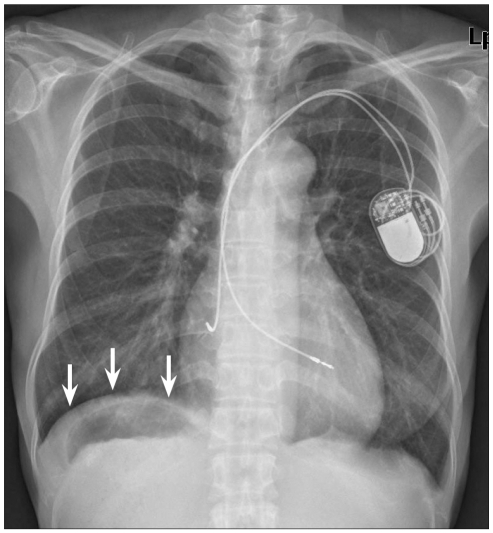
Fig. 4 The chest X-ray of 52-year-old woman showed gastric air under the right side of diaphragm (arrows), and hepatic shadow in the left side abnormally.

Fig. 5 Liver dynamic computed tomography. A: There were midline symmetric liver (L) and multiple spleens (black stars) and stomach (S) are located at the right side of abdomen. B: Multiple sandy stones in midline gallbladder. Superior mesenteric vein was unusually located anterior to the superior mesenteric artery. C: The left sided inferior vena cava was crossing the aorta at the level of diaphragm and was drained to right atrium. D: Liver was observed in both sides relative to midline.
Reference
-
1. Fulcher AS, Turner MA. Abdominal manifestations of situs anomalies in adults. Radiographics. 2002; 22:1439–1456. PMID: 12432114.2. Jacobs JP, Anderson RH, Weinberg PM, Walters HL 3rd, Tchervenkov CI, Del Duca D, Franklin RC, Aiello VD, Béland MJ, Colan SD, Gaynor JW, Krogmann ON, Kurosawa H, Maruszewski B, Stellin G, Elliott MJ. The nomenclature, definition and classification of cardiac structures in the setting of heterotaxy. Cardiol Young. 2007; 17(Suppl 2):1–28. PMID: 18039396.3. Brandenburg VM, Krueger S, Haage P, Mertens P, Riehl J. Heterotaxy syndrome with severe pulmonary hypertension in an adult. South Med J. 2002; 95:536–538. PMID: 12005012.4. Rose V, Izukawa T, Moës CA. Syndromes of asplenia and polysplenia. A review of cardiac and non-cardiac malformations in 60 cases withspecial reference to diagnosis and prognosis. Br Heart J. 1975; 37:840–852. PMID: 1191445.5. Gatrad AR, Read AP, Watson GH. Consanguinity and complex cardiac anomalies with situs ambiguus. Arch Dis Child. 1984; 59:242–245. PMID: 6712272.6. Peoples WM, Moller JH, Edwards JE. Polysplenia: a review of 146 cases. Pediatr Cardiol. 1983; 4:129–137. PMID: 6878069.7. Pepes S, Zidere V, Allan LD. Prenatal diagnosis of left atrial isomerism. Heart. 2009; 95:1974–1977. PMID: 19304670.8. Cho YH, Jin SJ, Je HC, Yoon YW, Hong BK, Kwon HM, Kim TH, Rim SJ. A case of noncompaction of the ventricular myocardium combined with situs ambiguous with polysplenia. Yonsei Med J. 2007; 48:1052–1055. PMID: 18159602.9. Sohn GH, Byun KM, Han HJ, Kim HJ, Choi JO, Lee SC, Park SW. A case of coarctation of aorta with left isomerism associated with inferior vena cava interruption and polysplenia. J Cardiovasc Ultrasound. 2007; 15:27–29.10. Kim JH, Seo HI, Kim HS, Kim DH, Jeon TY, Song GA, Kim S. Heterotaxia syndrome with intraluminal duodenal diverticulum. J Korean Surg Soc. 2010; 79:75–78.11. Cheon IS, Rhee YP, Choi BR, Lee SS, Jung WT, Lee JD, Choi DJ, Hwang JY, Seo BG, You JJ. Hemiazygos continuation of left inferior vena cava draining into the right atrium via persistent left superior vena cava: a variant of polysplenia syndrome mimicking aortic dissection. Korean Circ J. 1998; 28:440–447.12. Park YB, Kim JI, Cheung DY, Cho SH, Park SH, Han JY, Kim JK. A case of multiple intraabdominal anomalies including nonrotation of the intestine and a preduodenal portal vein. Korean J Med. 2007; 73:548–551.13. Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: imaging of the heterotaxy syndrome. Radiographics. 1999; 19:837–852. discussion 853-4. PMID: 10464794.14. Bartram U, Fischer G, Kramer HH. Congenitally interrupted inferior vena cava without other features of the heterotaxy syndrome: report of five cases and characterization of a rare entity. Pediatr Dev Pathol. 2008; 11:266–273. PMID: 17378673.15. Miranda R, Simpson CS, Nolan RL, Diez JC, Michael KA, Redfearn DP, Baranchuk A. Superior approach for radiofrequency ablation of atrio-ventricular nodal reentrant tachycardia in a patient with anomalous inferior vena cava and azygos continuation. Europace. 2010; 12:908–909. PMID: 20207745.16. Lee S, Cha JH, Han DH. Persistent left superior caval vein with absent right superior caval vein: importance of awareness. Cardiol Young. 2011; 1–3.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Situs Ambiguous with Polysplenia of Macrosomia
- Clinical Manifestation and Associated Cardiac Anomalies of Dextrocardia
- A Case of Noncompaction of the Ventricular Myocardium Combined with Situs Ambiguous with Polysplenia
- Anomalies of Abdominal Organs in Polysplenia Syndrome: Multidetector Computed Tomography Findings
- MR evaluation of visceroatrial situs abnormality
