Right Ventricular Compression Observed in Echocardiography from Pectus Excavatum Deformity
- Affiliations
-
- 1Department of Surgery, Division Cardiothoracic Surgery, Mayo Clinic Arizona, Phoenix, AZ, USA. Jaroszewski.dawn@mayo.edu
- 2Department of Medicine, Division of Cardiovascular Diseases, Mayo Clinic Arizona, Phoenix, AZ, USA.
- KMID: 1980381
- DOI: http://doi.org/10.4250/jcu.2011.19.4.192
Abstract
- Pectus excavatum exists as varying anatomic deformities and compression of the right heart by the chest wall can lead to patient symptoms including dyspnea and chest pain with exertion. Echocardiography can be difficult but is critical to the evaluation and diagnosis of this patient population. Modifying standard views such as biplane transthoracic and 3-D transesophageal views may be necessary in some patients due to limitations from the abnormal anatomy of the deformed anterior chest wall. Apical four-chamber views when seen clearly can usually visualize any extrinsic compression to the right ventricle of the heart.
Keyword
MeSH Terms
Figure
-
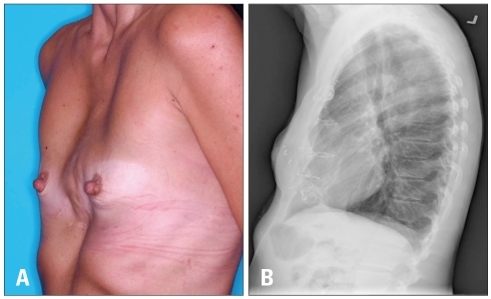
Fig. 1 A: Patient clinical photograph at physical examination demonstrating physical abnormality of the post-operative chest. B: Preoperative chest roentgenogram shows abnormal bony projection of sternum posterior

Fig. 2 Computed tomography with contrast showing bony projection of the deformed chest wall compressing the right ventricle (arrow).
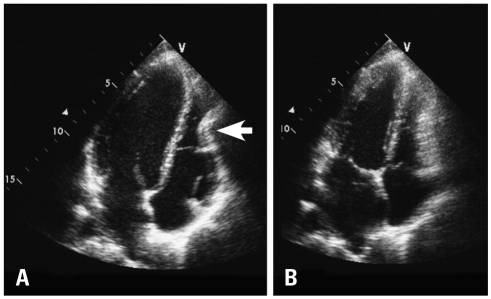
Fig. 3 Transthoracic echocardiography. Apical 4-chamber view demonstrates compression and deformation of the lower mid right ventricle by the chest wall in diastole which is more obvious during diastole (arrow) (A) than systole (B).
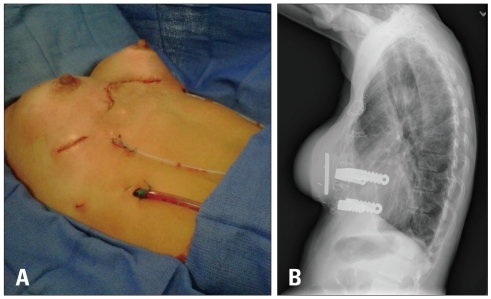
Fig. 4 A: Post surgical patient's chest was straightened and elevated 3-4 cm anterior to the heart and mediastinum with good cosmetic results and relief of cardiac compression. B: Lateral chest roentgenoram shows metal support bars and trabecular metal implant used to reconstruct patient's chest wall.
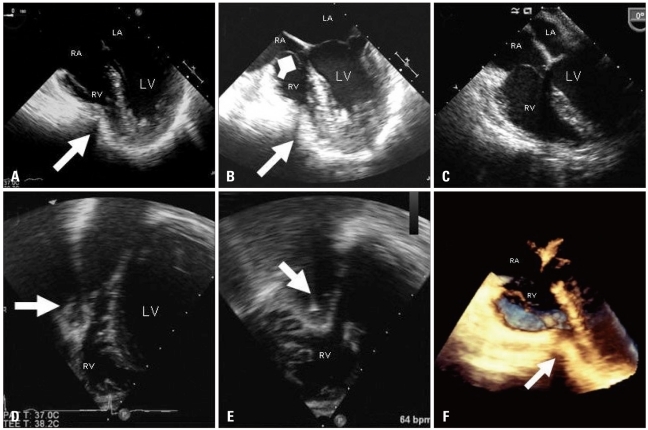
Fig. 5 Pre-operative transesophageal views showing extrinsic compassion of the RV during diastole (arrow) (A) and systole (arrow) (B). Tricuspid valve prolapse is evident during systole likely related to some distortion of the tricuspid annulus from extrinsic compression of the RV (square arrow) (B). Post-operative transesophageal image showing resolution of extrinsic RV compression (C). Note slight improvement in tricuspid valve prolapse as well following surgery. Pre-operative biplane images using three dimensional transesophageal probe from transgastric window showing extrinsic compression of the RV in the short axis (D) and long-axis views of the right ventricle simultaneously (arrows) (E). Note the acoustic shadowing behind the RV indentation due to bony structure. Improved visualization of the indentation of the right ventricle from live three dimensional image (arrow) (F). LV: left ventricle, LA: left atrium, RV: right ventricle, RA: right atrium.
Reference
-
1. Heinle J, Sabiston DC Jr. Sabiston DC, Lyerly HK, editors. Congenital deformities of the chest wall. Textbook of surgery: the biological basis of modern surgical practice. 1997. 15th ed. Philadelphia: WB Saunders Co;p. 1888–1896.2. Fokin AA, Steuerwald NM, Ahrens WA, Allen KE. Anatomical, histologic, and genetic characteristics of congenital chest wall deformities. Semin Thorac Cardiovasc Surg. 2009; 21:44–57. PMID: 19632563.3. Jaroszewski D, Notrica D, McMahon L, Steidley DE, Deschamps C. Current management of pectus excavatum: a review and update of therapy and treatment recommendations. J Am Board Fam Med. 2010; 23:230–239. PMID: 20207934.4. Jaroszewski DE, Fonkalsrud EW. Repair of pectus chest deformities in 320 adult patients: 21 year experience. Ann Thorac Surg. 2007; 84:429–433. PMID: 17643611.5. Jaroszewski D, Steidley E, Galindo A, Arabia F. Treating heart failure and dyspnea in a 78-year-old man with surgical correction of pectus excavatum. Ann Thorac Surg. 2009; 88:1008–1010. PMID: 19699946.6. Park SY, Park TH, Kim JH, Baek HK, Seo JM, Kim WJ, Nam YH, Cha KS, Kim MH, Kim YD. A case of right ventricular dysfunction caused by pectus excavatum. J Cardiovasc Ultrasound. 2010; 18:62–65. PMID: 20706572.7. Coln E, Carrasco J, Coln D. Demonstrating relief of cardiac compression with the Nuss minimally invasive repair for pectus excavatum. J Pediatr Surg. 2006; 41:683–686. discussion 683-6. PMID: 16567176.8. Krueger T, Chassot PG, Christodoulou M, Cheng C, Ris HB, Magnusson L. Cardiac function assessed by transesophageal echocardiography during pectus excavatum repair. Ann Thorac Surg. 2010; 89:240–243. PMID: 20103244.9. Mocchegiani R, Badano L, Lestuzzi C, Nicolosi GL, Zanuttini D. Relation of right ventricular morphology and function in pectus excavatum to the severity of the chest wall deformity. Am J Cardiol. 1995; 76:941–946. PMID: 7484836.10. Hawkins JA, Ehrenhaft JL, Doty DB. Repair of pectus excavatum by sternal eversion. Ann Thorac Surg. 1984; 38:368–373. PMID: 6486951.11. Raggi P, Callister TQ, Lippolis NJ, Russo DJ. Is mitral valve prolapse due to cardiac entrapment in the chest Cavity? A CT view. Chest. 2000; 117:636–642. PMID: 10712985.12. Fonkalsrud EW. Open repair of pectus excavatum with minimal cartilage resection. Ann Surg. 2004; 240:231–235. PMID: 15273545.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiac Cachexia Caused by Right Ventricular Outflow Tract Obstruction in a Patient With Severe Pectus Excavatum
- A Case of Right Ventricular Dysfunction Caused by Pectus Excavatum
- Repair of Recurrent Pectus Excavatum with a Huge Chest Wall Defect in a Patient with a Previous Ravitch and Pectus Bar Repair: A Case Report
- Development of New Cardiac Deformity Indexes for Pectus Excavatum on Computed Tomography: Feasibility for Pre- and Post-Operative Evaluation
- Embarrassed Radiofrequency Catheter Ablation of Supraventricular Tachycardia in Pectus Excavatum
