Validation of Three-Dimensional Echocardiography for Quantification of Aortic Root Geometry: Comparison with Multi-Detector Computed Tomography
- Affiliations
-
- 1Department of Cardiology, Ajou University School of Medicine, Suwon, Korea. shinjh@ajou.ac.kr
- KMID: 1980366
- DOI: http://doi.org/10.4250/jcu.2011.19.3.128
Abstract
- BACKGROUND
Three-dimensional (3D) echocardiography has been reported to be valuable for evaluating the geometry of cardiac chambers. We validated the accuracy of 3D transthoracic echocardiography for quantifying aortic root geometry in comparison with cardiac multi-detector computed tomography (MDCT).
METHODS
Twenty-three patients who underwent cardiac MDCT and showed normal left ventricular ejection fraction (> 55%), as assessed by 2-dimensional transthoracic echocardiography, were enrolled (12 male, mean 53 +/- 9 years). We defined the aortic root volume as the volume from the aortic annulus to the sinotubular junction. The aortic root volume at end-diastole measured by both cardiac MDCT and 3D echocardiography was assessed.
RESULTS
The cross-sectional area of the aortic root was asymmetric. At the annulus level, the cross-sectional area showed asymmetric triangle. From the aortic annulus to the most dilated point of the sinus of Valsalva, the asymmetric triangular shape was maintained. From the most dilated point of the sinus of Valsalva to the sinotubular junction, the cross-sectional shape of the aortic root changed to oval. The average aortic root volumes measured by 3D echocardiography (ARV-3DE) were 13.6 +/- 4.8 mL at end-diastole and 14.1 +/- 5.3 mL at end-systole, respectively. The average aortic root volume measured by MDCT at end-diastole (ARV-CT) was 14.1 +/- 5.7 mL. At end-diastole, the ARV-3DE correlated well with the ARV-CT (R2 = 0.926, difference = 0.5 +/- 1.7 mL), and the two methods were in excellent agreement (the percent difference was 0%).
CONCLUSION
Our results demonstrate both the feasibility and accuracy of 3D echocardiography for the clinical assessment of the geometry of the aortic root.
Keyword
MeSH Terms
Figure
-
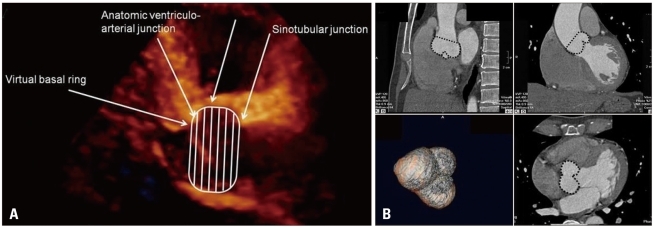
Fig. 1 Definition of the aortic root volume. The aortic root volume was defined as the volume from the aortic annulus to the sinotubular junction. The aortic annulus is defined at the level of the basal attachment of the aortic valve leaflets (i.e. the "inferior virtual basal ring"). The sinotubular junction is the interface between the aortic root and the tubular ascending aorta. A: Aortic root volume in three-dimensional echocardiography was measured in the parasternal long axis view. B: Aortic root volume in cardiac multi-detector computed tomography was measured using the multiplanar reconstructive method in the Vitrea2 imaging software.
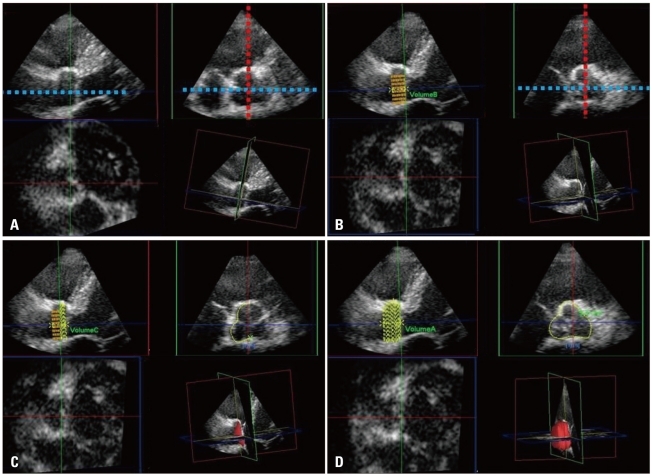
Fig. 2 Off-line analysis for quantification of the aortic root volume by 3-dimensional echocardiography. One plane (blue line) was aligned with the parallel line of the long axis of the ascending aorta passing the coaptation point of the aortic cusps. A second plane (red line) was set as the line perpendicular on the first line and cut across the coaptation point of the aortic cusps. The images of the parasternal long axis view were reversed due to limitation of the software we used. In order to acquire the most accurate aortic root volume data considering manipulation of the manual contour correction, the reversed images were chosen (A). From the aortic annulus to the sinotubular junction, 20 default slices were set. The aortic root was equally divided along the first line into 20 slices (B). The contours of each slice were traced as the inner layer of the aortic root manually (C). After defining the contour of each slice, the volume was calculated automatically using integration of each area (D).

Fig. 3 The geometric pattern of the aortic root cross-sectional area by three-dimensional echocardiography. A: Asymmetric triangular shape of the aortic annulus level. B: Asymmetric triangular shape at the most dilated portion of the sinus of Valsalva. C: Change of the geometry from asymmetric triangular to oval shape between the most dilated portion of the sinus of Valsalva to the sinotubular junction. D: Oval shape at the sinotubular junction.
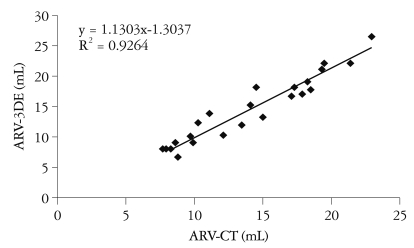
Fig. 4 Linear regression analysis for the three-dimensional echocardiography method versus the cardiac multi-detector computed tomography in quantification of the aortic root geometry. ARV-CT: the aortic root volume measured by computed tomography, ARV-3DE: the aortic root volume measured by three-dimensional echocardiography.
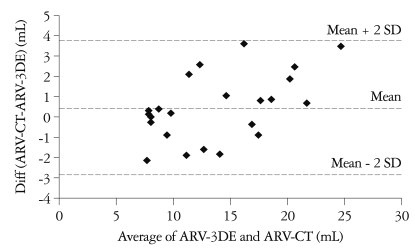
Fig. 5 Bland-Altman analysis for the three-dimensional echocardiography method versus the cardiac multi-detector computed tomography in quantification of the aortic root geometry. ARV-CT: the aortic root volume measured by computed tomography, ARV-3DE: the aortic root volume measured by three-dimensional echocardiography, SD: standard deviation.
Reference
-
1. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006; 368:1005–1011. PMID: 16980116.2. Anderson RH, Lal M, Ho SY. Anatomy of the aortic root with particular emphasis on options for its surgical enlargement. J Heart Valve Dis. 1996; 5(Suppl 3):S249–S257. PMID: 8953449.3. Lansac E, Lim HS, Shomura Y, Lim KH, Rice NT, Goetz W, Acar C, Duran CM. A four-dimensional study of the aortic root dynamics. Eur J Cardiothorac Surg. 2002; 22:497–503. PMID: 12297162.4. Tops LF, Wood DA, Delgado V, Schuijf JD, Mayo JR, Pasupati S, Lamers FP, van der Wall EE, Schalij MJ, Webb JG, Bax JJ. Noninvasive evaluation of the aortic root with multislice computed tomography implications for transcatheter aortic valve replacement. JACC Cardiovasc Imaging. 2008; 1:321–330. PMID: 19356444.5. Cheng A, Dagum P, Miller DC. Aortic root dynamics and surgery: from craft to science. Philos Trans R Soc Lond B Biol Sci. 2007; 362:1407–1419. PMID: 17594968.6. Akhtar M, Tuzcu EM, Kapadia SR, Svensson LG, Greenberg RK, Roselli EE, Halliburton S, Kurra V, Schoenhagen P, Sola S. Aortic root morphology in patients undergoing percutaneous aortic valve replacement: evidence of aortic root remodeling. J Thorac Cardiovasc Surg. 2009; 137:950–956. PMID: 19327523.7. Gopal AS, Keller AM, Rigling R, King DL Jr, King DL. Left ventricular volume and endocardial surface area by three-dimensional echocardiography: comparison with two-dimensional echocardiography and nuclear magnetic resonance imaging in normal subjects. J Am Coll Cardiol. 1993; 22:258–270. PMID: 8509549.8. Ota T, Kisslo J, von Ramm OT, Yoshikawa J. Real-time, volumetric echocardiography: usefulness of volumetric scanning for the assessment of cardiac volume and function. J Cardiol. 2001; 37(Suppl 1):93–101. PMID: 11433835.9. Ota T, Fleishman CE, Strub M, Stetten G, Ohazama CJ, von Ramm OT, Kisslo J. Real-time, three-dimensional echocardiography: feasibility of dynamic right ventricular volume measurement with saline contrast. Am Heart J. 1999; 137:958–966. PMID: 10220647.10. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986; 1:307–310. PMID: 2868172.11. Lansac E, Lim HS, Shomura Y, Lim KH, Rice NT, Goetz WA, Duran CM. Aortic root dynamics are asymmetric. J Heart Valve Dis. 2005; 14:400–407. PMID: 15974536.12. Rankin JS, Dalley AF, Crooke PS, Anderson RH. A 'hemispherical' model of aortic valvar geometry. J Heart Valve Dis. 2008; 17:179–186. PMID: 18512488.13. Delgado V, Schuijf JD, Bax JJ. Pre-operative aortic valve implantation evaluation: multimodality imaging. EuroIntervention. 2010; 6(Suppl G):G38–G47. PMID: 20542827.14. Binder T. Three-dimensional echocardiography: principles and promises. J Clin Basic Cardiol. 2002; 5:149–152.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Echocardiographic Preoperative Prediction of Prosthetic Aortic Valve Size in Patient with Aortic Valve Replacment
- Multi-Detector Row CT of the Central Airway Disease
- Advances in the Evaluation of Mitral Complex Geometry:Insights from Transthoracic Real-time Three-dimensional Echocardiography
- Contrast Echocardiography in two-dimensional left ventricular measurements: comparison with 256-row multi-detector computed tomography as a reference standard in Beagles
- Assessment of Right Ventricular Function in Pulmonary Hypertension with Multimodality Imaging
