Assessment of bifid and trifid mandibular canals using cone-beam computed tomography
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology, School of Dentistry, Mongolian National University Medical Science, Ulaanbaatar, Mongolia.
- 2Department of Oral and Maxillofacial Radiology, Dankook University College of Dentistry, Cheonan, Korea. ekkim@dankook.ac.kr
- KMID: 1974487
- DOI: http://doi.org/10.5624/isd.2014.44.3.229
Abstract
- PURPOSE
To investigate the prevalence of bifid and trifid mandibular canals using cone-beam computed tomography (CBCT) images, and to measure their length, diameter, and angle.
MATERIALS AND METHODS
CBCT images of 500 patients, involving 755 hemi-mandibles, were used for this study. The presence and type of bifid mandibular canal was evaluated according to a modified classification of Naitoh et al. Prevalence rates were determined according to age group, gender, and type. Further, their diameter, length, and angles were measured using PACSPLUS Viewer and ImageJ 1.46r. Statistical analysis with chi-squared and analysis of variance (ANOVA) tests was performed.
RESULTS
Bifid and trifid mandibular canals were found in 22.6% of the 500 patients and 16.2% of the 755 sides. There was no significant difference between genders and among age groups. The retromolar canal type accounted for 71.3% of the identified canals; the dental canal type, 18.8%; the forward canal type, 4.1%; and the trifid canal type, 5.8%. Interestingly, seven cases of the trifid canal type, which has been rarely reported, were observed. The mean diameter of the bifid and trifid mandibular canals was 2.2 mm and that of the main mandibular canal was 4.3 mm. Their mean length was 16.9 mm; the mean superior angle was 149.2degrees, and the mean inferior angle was 37.7degrees.
CONCLUSION
Bifid and trifid mandibular canals in the Korean population were observed at a relatively high rate through a CBCT evaluation, and the most common type was the retromolar canal. CBCT is suggested for a detailed evaluation of bifid and trifid mandibular canals before mandibular surgery.
MeSH Terms
Figure
-

Fig. 1 Cone-beam computed tomography (CBCT) image shows canal type 1 (retromolar canal type).
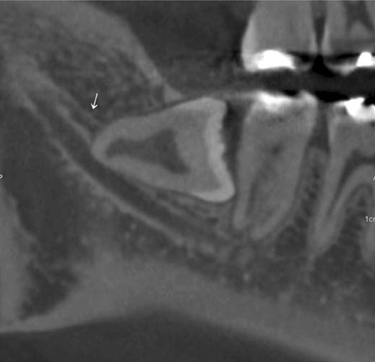
Fig. 2 CBCT image shows canal type 2 (dental canal type).
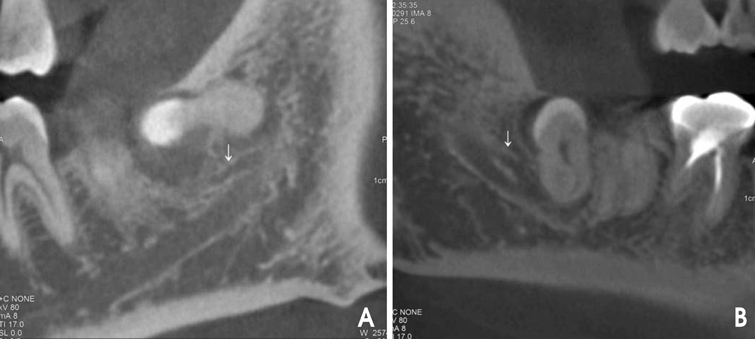
Fig. 3 CBCT images show canal type 3 (forward canal type A without confluence, B with confluence).

Fig. 4 CBCT image shows canal type 5A (trifid canal type: two accessory canals of the retromolar canal type).
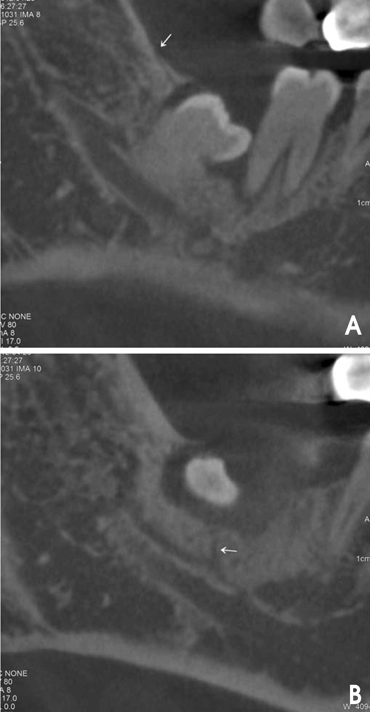
Fig. 5 CBCT images show canal type 5B (trifid canal type: two accessory canals of one retromolar (A) and one dental canal (B) type).

Fig. 6 CBCT image shows canal type 5C (trifid canal type: two accessory canals of the dental canal type).
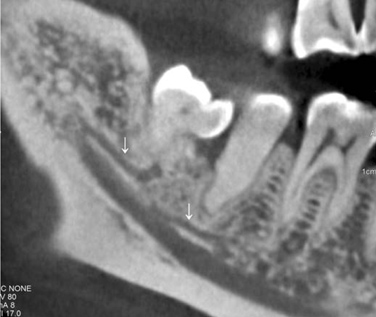
Fig. 7 CBCT image shows canal type 5D (trifid canal type: two accessory canals of one dental and one forward canal type).
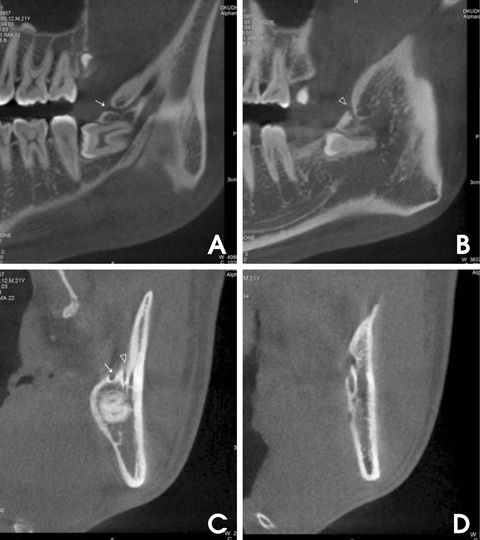
Fig. 8 CBCT images show canal type 5E (trifid canal type: two accessory canals of the retromolar canal type (A-C) with two mandibular foramina (D)).
Cited by 1 articles
-
A rare case of trifid mandibular canal with bilateral retromolar foramina
Quang Do, Daniel Shen, Hiroe Ohyama, R. Shane Tubbs, Joe Iwanaga
Anat Cell Biol. 2020;53(4):512-515. doi: 10.5115/acb.20.153.
Reference
-
1. Naitoh M, Hiraiwa Y, Aimiya H, Ariji E. Observation of bifid mandibular canal using cone-beam computerized tomography. Int J Oral Maxillofac Implants. 2009; 24:155–159.2. Langlais RP, Broadus R, Glass BJ. Bifid mandibular canals in panoramic radiographs. J Am Dent Assoc. 1985; 110:923–926.
Article3. Carter RB, Keen EN. The intra mandibular course of the inferior alveolar nerve. J Anat. 1971; 108:433–440.4. Nortjé CJ, Farman AG, Grotepass FW. Variations in the normal anatomy of the inferior dental (mandibular) canal: a retrospective study of panoramic radiographs from 3612 routine dental patients. Br J Oral Surg. 1977; 15:55–63.
Article5. Bogdán S, Pataky L, Barabás J, Németh Z, Huszár T, Szabò G. Atypical courses of the mandibular canal: comparative examination of dry mandibles and x-rays. J Craniofac Surg. 2006; 17:487–491.6. Auluck A, Pai KM, Mupparapu M. Multiple mandibular nerve canals: radiographic observations and clinical relevance. Report of 6 cases. Quintessence Int. 2007; 38:781–787.7. Wadhwani P, Mathur RM, Kohli M, Sahu R. Mandibular canal variant: a case report. J Oral Pathol Med. 2008; 37:122–124.
Article8. Grover PS, Lorton L. Bifid mandibular nerve as a possible cause of inadequate anesthesia in the mandible. J Oral Maxillofac Surg. 1983; 41:177–179.
Article9. Juodzbalys G, Wang HL, Sabalys G. Anatomy of mandibular vital structures. Part 1: mandibular canal and inferior alveolar neurovascular bundle in relation with dental implantology. J Oral Maxillofac Res. 2010; 1:e2.
Article10. Claeys V, Wackens G. Bifid mandibular canal: literature review and case report. Dentomaxillofac Radiol. 2005; 34:55–58.
Article11. Naitoh M, Hiraiwa Y, Aimiya H, Gotoh M, Ariji Y, Izumi M, et al. Bifid mandibular canal in Japanese. Implant Dent. 2007; 16:24–32.
Article12. Rouas P, Nancy J, Bar D. Identification of double mandibular canals: literature review and three case reports with CT scans and cone beam CT. Dentomaxillofac Radiol. 2007; 36:34–38.
Article13. Lee JS, Yoon SJ, Kang BC. Mandibular canal branches supplying the mandibular third molar observed on cone beam computed tomographic images: reports of four cases. Korean J Oral Maxillofac Radiol. 2009; 39:209–212.14. Lee HW, Kim YG, Lee BS, Kwon YD, Choi BJ, Kim YR. Bifid mandibular canal: radiographic observation and clinical relevance - a case report. J Korean Dent Soc Anesthesiol. 2009; 9:24–29.15. Kuribayashi A, Watanabe H, Imaizumi A, Tantanapornkul W, Katakami K, Kurabayashi T. Bifid mandibular canals: cone beam computed tomography evaluation. Dentomaxillofac Radiol. 2010; 39:235–239.
Article16. Orhan K, Aksoy S, Bilecenoglu B, Sakul BU, Paksoy CS. Evaluation of bifid mandibular canals with cone-beam computed tomography in a Turkish adult population: a retrospective study. Surg Radiol Anat. 2011; 33:501–507.
Article17. de Oliveira-Santos C, Souza PH, de Azambuja Berti-Couto S, Stinkens L, Moyaert K, Rubira-Bullen IR, et al. Assessment of variations of the mandibular canal through cone beam computed tomography. Clin Oral Investig. 2012; 16:387–393.
Article18. Mizbah K, Gerlach N, Maal TJ, Bergé SJ, Meijer GJ. The clinical relevance of bifid and trifid mandibular canals. Oral Maxillofac Surg. 2012; 16:147–151.
Article19. Fu E, Peng M, Chiang CY, Tu HP, Lin YS, Shen EC. Bifid mandibular canals and the factors associated with their presence: a medical computed tomography evaluation in a Taiwanese population. Clin Oral Implants Res. 2014; 25:e64–e67.
Article20. Kang JH, Lee KS, Oh MG, Choi HY, Lee SR, Oh SH, et al. The incidence and configuration of the bifid mandibular canal in Koreans by using cone-beam computed tomography. Imaging Sci Dent. 2014; 44:53–60.
Article21. Naitoh M, Nakahara K, Suenaga Y, Gotoh K, Kondo S, Ariji E. Comparison between cone-beam and multislice computed tomography depicting mandibular neurovascular canal structures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 109:e25–e31.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The incidence and configuration of the bifid mandibular canal in Koreans by using cone-beam computed tomography
- Mandibular canal branches supplying the mandibular third molar observed on cone beam computed tomographic images: Reports of four cases
- Cone beam CT findings of retromolar canals: Report of cases and literature review
- Assessment of the relationship between the mandibular third molar and the mandibular canal using panoramic radiograph and cone beam computed tomography
- Accuracy verification of dental cone-beam computed tomography of mandibular incisor root canals and assessment of its morphology and aging-related changes
