Aneurysmal bone cyst of the mandible managed by conservative surgical therapy with preoperative embolization
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology, School of Dentistry, Kyungpook National University, Daegu, Korea. syan@knu.ac.kr
- KMID: 1974405
- DOI: http://doi.org/10.5624/isd.2012.42.1.35
Abstract
- A 9-year-old girl visited our hospital, complaining of a rapid-growing and rigid swelling on the left posterior mandibular area. Panoramic radiograph showed a moderately defined multilocular honeycomb appearance involving the left mandibular body. CT scan revealed an expansile, multilocular osteolytic lesion and multiple fluid levels within cystic spaces. Bone scan demonstrated increased radiotracer uptake and angiography showed a highly vascularized lesion. The lesion was suspected as aneurysmal bone cyst (ABC) and preoperative embolization was performed, which minimize the extent of operation and the surgical complication. The lesion was treated by surgical curettage and lateral decortication with repositioning. No additional treatment such as a surgical reconstruction or bone graft was needed. Early diagnosis of ABC is very important and appropriate treatment should be performed considering several factors such as age, surgical complication, and possibility of recurrence.
MeSH Terms
Figure
-
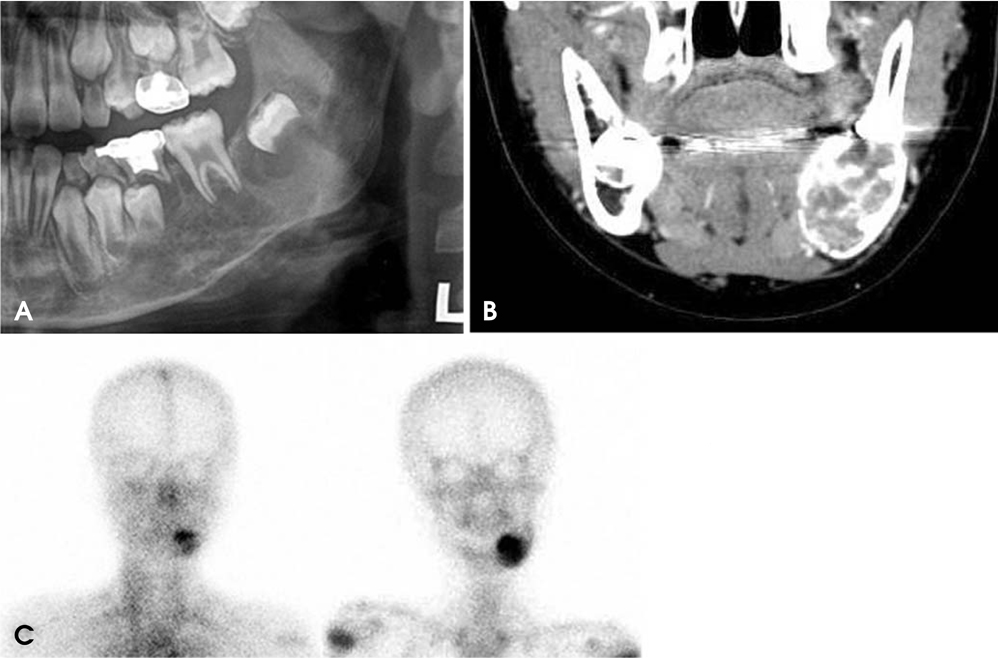
Fig. 1 A. Cropped panoramic radiograph reveals multilocular honeycomb appearance with expansion of cortical bone on the left mandibular body area. B. Coronal contrast enhanced CT scan shows an expansile, multilocular osteolytic lesion with multiple internal septation and multiple fluid levels within cystic spaces at the left mandible. C. The blood-pool (left) and delayed phase (right) reveal an increased radiotracer uptake in the left mandibular body area.
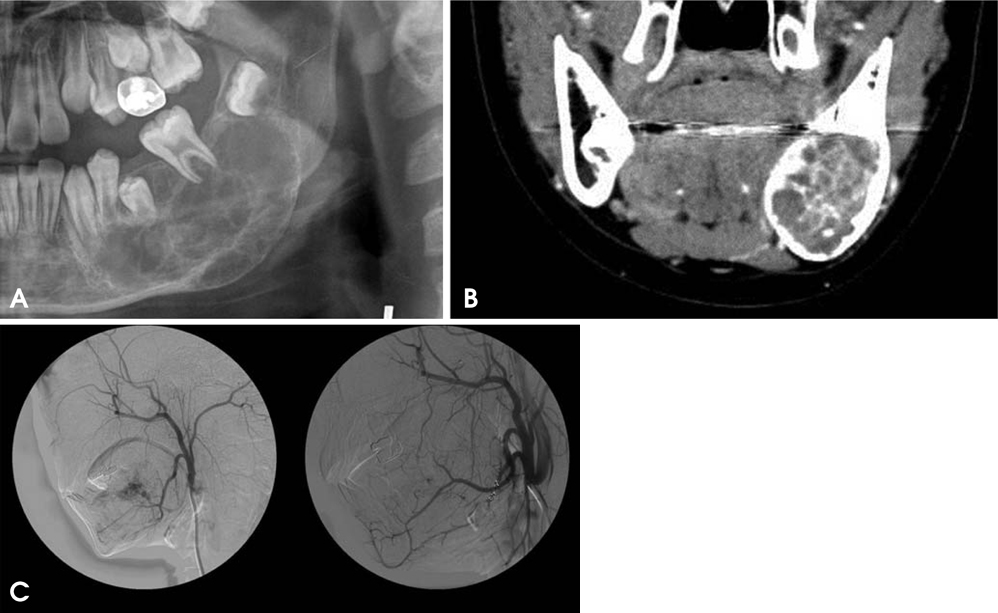
Fig. 2 A. Cropped panoramic radiograph shows that the lesion grows largely and the internal septa show multilocular soap bubble appearance five months later. B. Coronal contrast enhanced CT image shows the similar features compared with the previous CT images but enlarged lesion. C. Pre-embolization angiogram demonstrates a highly vascularized lesion (left). Post-angiogram shows occlusion of the feeder vessel (right).

Fig. 3 The buccal cortex is decorticated (left) and the inferior alveolar nerve is preserved during curettage (right).
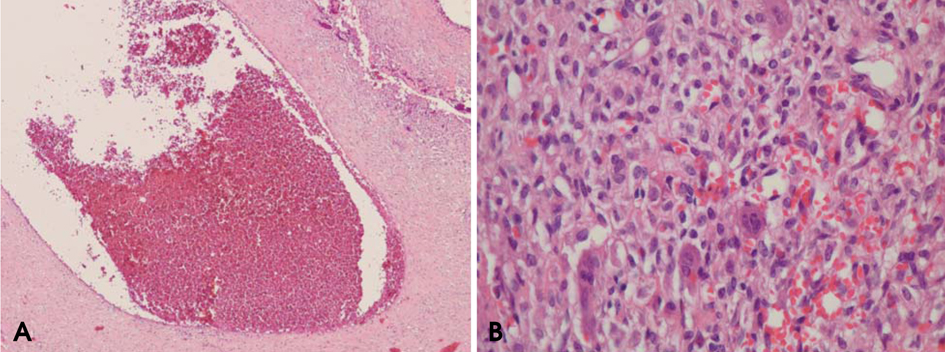
Fig. 4 A. Histopathologic examination reveals sinusoidal spaces filled with red blood cells (H&E stain, ×40). B. A multinucleated osteoclast type of giant cell is in fibrous tissue (H&E stain, ×400).
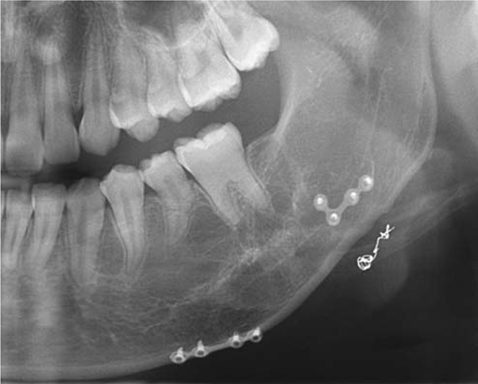
Fig. 5 Cropped panoramic radiograph taken 5.7 years after the operation shows a normal bony healing and no recurrence sign.
Reference
-
1. Breuer C, Paul H, Zimmermann A, Braunstein S, Schaper J, Mayatepek E, et al. Mandibular aneurysmal bone cyst in a child misdiagnosed as acute osteomyelitis: a case report and a review of the literature. Eur J Pediatr. 2010. 169:1037–1040.
Article2. Cottalorda J, Kohler R, Sales de Gauzy J, Chotel F, Mazda K, Lefort G, et al. Epidemiology of aneurysmal bone cyst in children: a multicenter study and literature review. J Pediatr Orthop B. 2004. 13:389–394.
Article3. Sun ZJ, Sun HL, Yang RL, Zwahlen RA, Zhao YF. Aneurysmal bone cysts of the jaws. Int J Surg Pathol. 2009. 17:311–322.4. Motamedi MH, Yazdi E. Aneurysmal bone cyst of the jaws: analysis of 11 cases. J Oral Maxillofac Surg. 1994. 52:471–475.5. Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst: with emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg. 1942. 44:1004–1025.6. Rosenberg AE, Nielsen GP, Fletcher JA. Fletcher CD, Unni KK, Mertens F, editors. Aneurysmal bone cyst. WHO classification of tumors: pathology and genetics of tumors of soft tissue and bone. 2005. 3rd ed. Lyon: IARC Press;338–339.7. Jundt G. Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Aneurysmal bone cyst. WHO classification of tumors: pathology and genetics of head and neck tumors. 2005. 3rd ed. Lyon: IARC Press;326.8. Wang K, Allen L, Fung E, Chan CC, Chan JC, Griffith JF. Bone scintigraphy in common tumors with osteolytic components. Clin Nucl Med. 2005. 30:655–671.
Article9. Kalantar Motamedi MH. Aneurysmal bone cysts of the jaws: clinicopathological features, radiographic evaluation and treatment analysis of 17 cases. J Craniomaxillofac Surg. 1998. 26:56–62.10. Motamedi MH, Navi F, Eshkevari PS, Jafari SM, Shams MG, Taheri M, et al. Variable presentations of aneurysmal bone cysts of the jaws: 51 cases treated during a 30-year period. J Oral Maxillofac Surg. 2008. 66:2098–2103.
Article11. Sun ZJ, Zhao YF, Yang RL, Zwahlen RA. Aneurysmal bone cysts of the jaws: analysis of 17 cases. J Oral Maxillofac Surg. 2010. 68:2122–2128.
Article12. Motamedi MH. Destructive aneurysmal bone cyst of the mandibular condyle: report of a case and review of the literature. J Oral Maxillofac Surg. 2002. 60:1357–1361.
Article13. White SC, Pharoah MJ. Oral radiology; principles and interpretation. 2009. 6th ed. St. Louis: Mosby-Year Book Inc;445–446.14. Hudson TM. Scintigraphy of aneurysmal bone cysts. AJR Am J Roentgenol. 1984. 142:761–765.
Article15. Seven B, Varoglu E, Alper F, Keles M, Koplay M. Aneurysmal bone cyst of the second metatarsal: three-phase bone scan findings and radiological assessment. Hell J Nucl Med. 2008. 11:189–190.16. Cottalorda J, Bourelle S. Modern concepts of primary aneurysmal bone cyst. Arch Orthop Trauma Surg. 2007. 127:105–114.
Article17. Khambete N, Risbud M, Mehta N. Interventional radiography in management of high-flow arteriovenous malformation of maxilla: report of a case. Imaging Sci Dent. 2011. 41:123–128.
Article18. Struthers PJ, Shear M. Aneurysmal bone cyst of the jaws. (I). Clinicopathological features. Int J Oral Surg. 1984. 13:85–91.19. Cottalorda J, Bourelle S. Current treatments of primary aneurismal bone cysts. J Pediatr Orthop B. 2006. 15:155–167.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transcatheter arterial embolization of Aneurysmal Bone Cyst in Pubic Bone: A Case Report
- Aneurysmal Bone Cyst in Clavicle: Report of A Case
- Aneurysamal bone cyst: report of a case
- Huge Aneurysmal Bone Cyst of the Sacrum: A Case Report
- Large Aneurysmal Bone Cyst of the Posterior Archofa Lumbar Vertebraina Child Treated with En Bloc Excision: A Case Report
