Endocrinol Metab.
2012 Dec;27(4):318-322. 10.3803/EnM.2012.27.4.318.
A Case of Latent Autoimmune Diabetes in Adults Developed after Surgical Cure of Growth Hormone Secreting Pituitary Tumor
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. edgo@yuhs.ac
- 2Institute of Endocrinology, Goodmorning Hospital, Pyeongtaek, Korea.
- 3Institute of Endocrinology, Gwangmyung Sungae Hospital, Gwangmyeong, Korea.
- 4Institute of Endocrine Research, Yonsei University College of Medicine, Seoul, Korea.
- 5Diabetes Center, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1973797
- DOI: http://doi.org/10.3803/EnM.2012.27.4.318
Abstract
- Acromegaly is generally caused by a benign growth hormone (GH)-secreting pituitary adenoma. It is characterized by a wide range of complications; cardiovascular, respiratory, bone and joint, and metabolic complications. Among them, impaired glucose tolerance and diabetes mellitus, due to GH-induced insulin resistance, has been reported in approximately 16-46% and 19-56%. They are usually improved following the treatment of acromegaly, surgical or medical therapy. We report a first case of 36-year-old man who was paradoxically diagnosed with GAD antibody positive latent autoimmune diabetes in adults (LADA) after the surgical cure of acromegaly.
Keyword
MeSH Terms
Figure
-
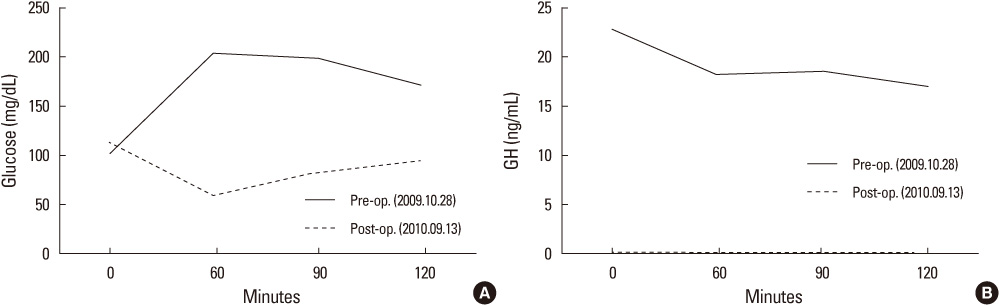
Fig. 1 A 75 g oral glucose tolerance tests (pre- and post-operation). (A) A 75 g oral glucose tolerance test for serum glucose levels; This patient was confirmed acromegaly with insulin-independent diabetes mellitus. It is cured after tumor resection. (B) A 75 g oral glucose tolerance test for growth hormone as a confirmation test for acromegaly remission. There was excessive secretion of growth hormone (GH) which was decreased after tumor resection (GH normal range, 0-9.5 ng/mL).
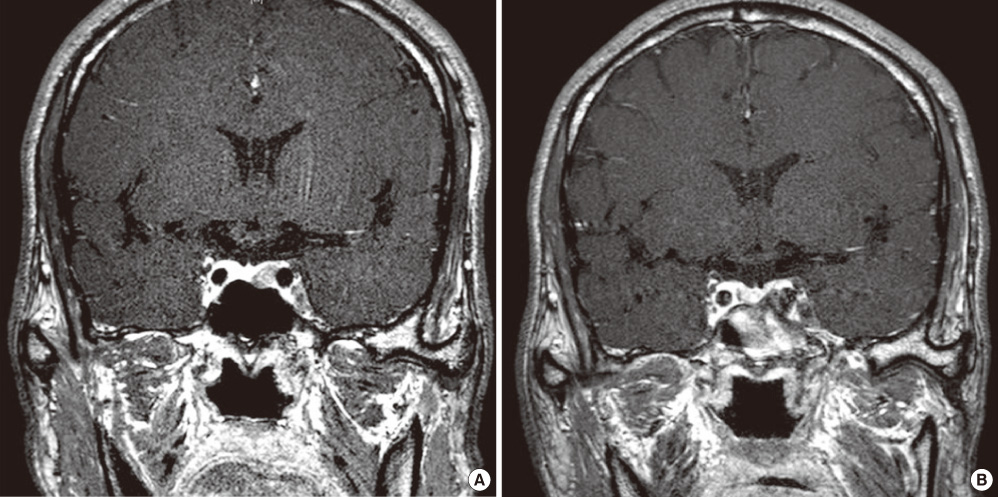
Fig. 2 Sella magnetic resonance imaging and dynamic. (A) Pre-operation (November 25, 2009). (B) One year after operation (March 9, 2011).
Reference
-
1. Yang IM. Clinical characteristics of acromegalic patients in Korea. J Korean Soc Endocrinol. 1994. 9:290–306.2. Kreze A, Kreze-Spirova E, Mikulecky M. Risk factors for glucose intolerance in active acromegaly. Braz J Med Biol Res. 2001. 34:1429–1433.3. Møller N, Schmitz O, Jøorgensen JO, Astrup J, Bak JF, Christensen SE, Alberti KG, Weeke J. Basal- and insulin-stimulated substrate metabolism in patients with active acromegaly before and after adenomectomy. J Clin Endocrinol Metab. 1992. 74:1012–1019.4. Scacchi M, Cavagnini F. Acromegaly. Pituitary. 2006. 9:297–303.5. Juneja R, Palmer JP. Type 1 1/2 diabetes: myth or reality? Autoimmunity. 1999. 29:65–83.6. Palmer JP, Hirsch IB. What's in a name: latent autoimmune diabetes of adults, type 1.5, adult-onset, and type 1 diabetes. Diabetes Care. 2003. 26:536–538.7. Kinoshita Y, Fujii H, Takeshita A, Taguchi M, Miyakawa M, Oyama K, Yamada S, Takeuchi Y. Impaired glucose metabolism in Japanese patients with acromegaly is restored after successful pituitary surgery if pancreatic {beta}-cell function is preserved. Eur J Endocrinol. 2011. 164:467–473.8. Ko KS, Hong SK, Lee KU, Kim NH, Choi DS, Ihm SH, Park SW, Kim CH, Byun DW, Suh KI, Chang HC, Rhee BD. The frequency of ICA and anti-GAD antibody in Korean IDDM and NIDDM patients. J Korean Diabetes Assoc. 1998. 22:312–319.9. Kim CS, Park J, Cho MH, Park JS, Nam JY, Kim DM, Ahn CW, Cha BS, Lim SK, Kim KR, Lee HC. Frequency of anti-GAD antibody in non-obese, adult-onset type 2 diabetes in Korea and clinical and biological characteristics according to anti-GAD antibody. J Korean Diabetes Assoc. 2004. 28:66–74.10. Cittadini A, Strömer H, Katz SE, Clark R, Moses AC, Morgan JP, Douglas PS. Differential cardiac effects of growth hormone and insulin-like growth factor-1 in the rat. A combined in vivo and in vitro evaluation. Circulation. 1996. 93:800–809.11. Ho KY, Weissberger AJ. The antinatriuretic action of biosynthetic human growth hormone in man involves activation of the renin-angiotensin system. Metabolism. 1990. 39:133–137.12. Fatti LM, Scacchi M, Pincelli AI, Lavezzi E, Cavagnini F. Prevalence and pathogenesis of sleep apnea and lung disease in acromegaly. Pituitary. 2001. 4:259–262.13. Jadresic A, Banks LM, Child DF, Diamant L, Doyle FH, Fraser TR, Joplin GF. The acromegaly syndrome. Relation between clinical features, growth hormone values and radiological characteristics of the pituitary tumours. Q J Med. 1982. 51:189–204.14. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2004. 27:Suppl 1. S5–S10.15. Seok H, Lee BW. Latent autoimmune diabetes in adults: autoimmune diabetes in adults with slowly progressive beta-cell failure. Diabetes Metab J. 2012. 36:116–119.16. Hwangbo Y, Kim JT, Kim EK, Khang AR, Oh TJ, Jang HC, Park KS, Kim SY, Lee HK, Cho YM. Prevalence and clinical characteristics of recently diagnosed type 2 diabetes patients with positive anti-glutamic Acid decarboxylase antibody. Diabetes Metab J. 2012. 36:136–143.17. Zimmet PZ. The pathogenesis and prevention of diabetes in adults. Genes, autoimmunity, and demography. Diabetes Care. 1995. 18:1050–1064.18. Naik RG, Brooks-Worrell BM, Palmer JP. Latent autoimmune diabetes in adults. J Clin Endocrinol Metab. 2009. 94:4635–4644.19. Nabarro JD. Acromegaly. Clin Endocrinol (Oxf). 1987. 26:481–512.20. Fonseca VA, Dandona P, Havard CW. Diabetes mellitus after hypophysectomy for acromegaly. Br Med J (Clin Res Ed). 1987. 294:413–414.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment Strategy of Growth Hormone Secreting Pituitary Adenoma
- A Case of Secondary Amenorrhea Associated with Pituitary Tumor
- Surgical Results of Growth Hormone-Secreting Pituitary Adenoma
- Result of Surgical Management of Pituitary Tumor
- Ectopic Growth Hormone-Secreting Pituitary Adenoma of the Clivus
