Indications and Short-term Results of Open Surgical Repair of Abdominal Aortic Aneurysm in an Endovascular Era
- Affiliations
-
- 1Division of Vascular Surgery, Department of Surgery, Samsung Medical Center (SMC), Sungkyunkwan University School of Medicine, Seoul, Korea. ywkim@skku.edu
- 2Department of Radiology, Samsung Medical Center (SMC), Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Cardiology, Samsung Medical Center (SMC), Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1963585
- DOI: http://doi.org/10.4174/jkss.2011.80.3.212
Abstract
- PURPOSE
To assess the role of OR in treatment of AAA patients, we reviewed the indications and our current results of OR of AAA.
METHODS
We retrospectively investigated the database of 366 patients (mean age, 68.3+/-8.7 years, male 86%) who underwent open surgical (n=291, 80%) or endovascular treatments (n=75, 20%) of AAA in a tertiary referral center between Sep. 2003 to Aug. 2010. Treatment-related morbidities and mortality rates within 30 days were investigated according to the indications for treatment, clinical features, anatomic location, and underlying causes of AAA.
RESULTS
According to the location of AAA, we treated 343 (94%) infrarenal, 17 (5%) juxtarenal and 6 (2%) suprarenal AAAs. Underlying causes of AAA were degenerative (90%), infected (3%), inflammatory (3%), Marfan's syndrome (2%), and vasculitis (0.5%). Clinically, 338 (92%) were non-ruptured and 28 (8%) were ruptured AAAs. 75% of patients were treated with OR after the inception of reimbursement of aortic device while 25% of patients were treated with EVARs. The operative mortality rates of OR was 0.4% in patients with non-ruptured infrarenal AAA, 0% in patients with non-ruptured juxta- and suprarenal AAA and 21.4% in ruptured AAA patients.
CONCLUSION
In an era of endovascular treatment of AAA, we have experienced excellent surgical results after OR in patients with non-ruptured AAA with various clinical features. Though EVAR is rapidly replacing OR in treatment of infrarenal AAAs, OR has its own role in treatment of AAA patients with unfavorable conditions for EVAR. The role of OR should not be underestimated.
Keyword
MeSH Terms
Figure
-
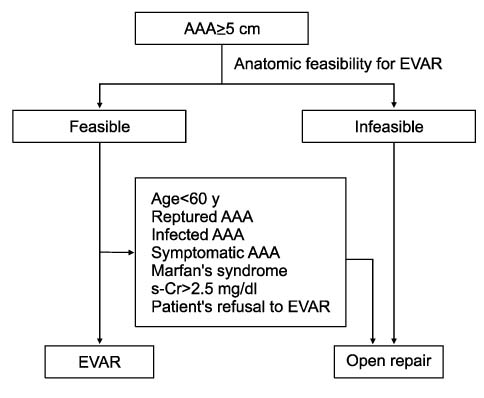
Fig. 1 Treatment algorithm for patients with abdominal aortic aneurysm (AAA).

Fig. 2 Result of preoperative cardiac evaluation before elective treatment of abdominal aortic aneurysm (AAA) (N=341). *Percutaneous coronary intervention; †Coronary artery bypass grafting.

Fig. 3 Indications for AAA treatment (Sep. 2003~Aug. 2010). *Thoracoabdominal aortic aneurysm.

Fig. 4 A patient who required open conversion during EVAR. (A) Completion angiogram during EVAR shows extravasation of contrast agent after deployment of the aortic stent graft with suprarenal fixing device. (B) An operative finding of ruptured abdominal aortic aneurysm (AAA) showing aortic stent graft. (C) Excised aortic stent graft device (Zenith®): suprarenal stents were removed during the operation. (D) Follow-up CT angiogram shows abdominal aortic and the left renal artery reconstructions.
Reference
-
1. Lloyd WE, Paty PS, Darling RC 3rd, Chang BB, Fitzgerald KM, Leather RP, et al. Results of 1000 consecutive elective abdominal aortic aneurysm repairs. Cardiovasc Surg. 1996. 4:724–726.2. Aune S. Risk factors and operative results of patients aged less than 66 years operated on for asymptomatic abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. 2001. 22:240–243.3. Starr JE, Hertzer NR, Mascha EJ, O'Hara PJ, Krajewski LP, Sullivan TM, et al. Influence of gender on cardiac risk and survival in patients with infrarenal aortic aneurysms. J Vasc Surg. 1996. 23:870–880.4. Nowygrod R, Egorova N, Greco G, Anderson P, Gelijns A, Moskowitz A, et al. Trends, complications, and mortality in peripheral vascular surgery. J Vasc Surg. 2006. 43:205–216.5. Giles KA, Pomposelli F, Hamdan A, Wyers M, Jhaveri A, Schermerhorn ML. Decrease in total aneurysm-related deaths in the era of endovascular aneurysm repair. J Vasc Surg. 2009. 49:543–550. discussion 50-1.6. Schwarze ML, Shen Y, Hemmerich J, Dale W. Age-related trends in utilization and outcome of open and endovascular repair for abdominal aortic aneurysm in the United States, 2001-2006. J Vasc Surg. 2009. 50:722.e2–729.e2.7. Lawrence PF, Gazak C, Bhirangi L, Jones B, Bhirangi K, Oderich G, et al. The epidemiology of surgically repaired aneurysms in the United States. J Vasc Surg. 1999. 30:632–640.8. Mureebe L, Egorova N, Giacovelli JK, Gelijns A, Kent KC, McKinsey JF. National trends in the repair of ruptured abdominal aortic aneurysms. J Vasc Surg. 2008. 48:1101–1107.9. Kim YC, Yun IJ, Ha JW, Yang HK, Ahn H, Kim SJ. 10 year experiences of surgically treated abdominal aortic aneurysm patients. J Korean Surg Soc. 1996. 12:167–175.10. Park YJ, Lee JH, Ha J, Chung JW, Park JH, Kim SJ. 118 cases of abdominal aortic aneurysm (AAA) repair. J Korean Surg Soc. 2003. 65:441–446.11. Prinssen M, Verhoeven EL, Buth J, Cuypers PW, van Sambeek MR, Balm R, et al. A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med. 2004. 351:1607–1618.12. Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomised controlled trial. Lancet. 2004. 364:843–848.13. Schermerhorn ML, O'Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon BE. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008. 358:464–474.14. Hertzer NR, Mascha EJ, Karafa MT, O'Hara PJ, Krajewski LP, Beven EG. Open infrarenal abdominal aortic aneurysm repair: the Cleveland Clinic experience from 1989 to 1998. J Vasc Surg. 2002. 35:1145–1154.15. Menard MT, Chew DK, Chan RK, Conte MS, Donaldson MC, Mannick JA, et al. Outcome in patients at high risk after open surgical repair of abdominal aortic aneurysm. J Vasc Surg. 2003. 37:285–292.16. Sicard GA, Reilly JM, Rubin BG, Thompson RW, Allen BT, Flye MW, et al. Transabdominal versus retroperitoneal incision for abdominal aortic surgery: report of a prospective randomized trial. J Vasc Surg. 1995. 21:174–181. discussion 81-3.17. Hannan EL, Kilburn H Jr, O'Donnell JF, Bernard HR, Shields EP, Lindsey ML, et al. A longitudinal analysis of the relationship between in-hospital mortality in New York State and the volume of abdominal aortic aneurysm surgeries performed. Health Serv Res. 1992. 27:517–542.18. Dardik A, Lin JW, Gordon TA, Williams GM, Perler BA. Results of elective abdominal aortic aneurysm repair in the 1990s: A population-based analysis of 2335 cases. J Vasc Surg. 1999. 30:985–995.19. Katz DJ, Stanley JC, Zelenock GB. Operative mortality rates for intact and ruptured abdominal aortic aneurysms in Michigan: an eleven-year statewide experience. J Vasc Surg. 1994. 19:804–815. discussion 16-7.20. Kazmers A, Jacobs L, Perkins A, Lindenauer SM, Bates E. Abdominal aortic aneurysm repair in Veterans Affairs medical centers. J Vasc Surg. 1996. 23:191–200.21. Dimick JB, Upchurch GR Jr. Endovascular technology, hospital volume, and mortality with abdominal aortic aneurysm surgery. J Vasc Surg. 2008. 47:1150–1154.22. Hosokawa Y, Takano H, Aoki A, Inami T, Ogano M, Kobayashi N, et al. Management of coronary artery disease in patients undergoing elective abdominal aortic aneurysm open repair. Clin Cardiol. 2008. 31:580–585.23. Tiefenbacher CP. Abdominal aortic aneurysm repair in cardiac high risk patients--medication, surgery or stent? Clin Res Cardiol. 2008. 97:215–221.24. Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, et al. ACC/AHA 2005 guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): executive summary a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease) endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. J Am Coll Cardiol. 2006. 47:1239–1312.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Stent-Graft Placement and Secondary Intervention for Abdominal Aortic Aneurysm in a Patient who had a Previously Inserted Iliac Stent
- Novel Technique to Rescue a Folded Aortic Endograft during Endovascular Aneurysm Repair
- Endovascular Repair of a Juxtarenal Abdominal Aortic Aneurysm Using a Chimney Graft
- Ruptured Abdominal Aortic Aneurysm with Antecedent Endovascular Repair of Abdominal Aortic Aneurysm
- Total Laparoscopic Abdominal Aortic Aneurysm Repair: A Case Report
