The Usefulness of the Frontolateral Approach as a Minimally Invasive Corridor for Clipping of Anterior Circulation Aneurysm
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Bundang Hospital, Seongnam, Korea. nsbang@snubh.org
- 2Department of Biological Engineering, Massachusetts Institute of Technology, Cambridge, MA, United States.
- KMID: 1963161
- DOI: http://doi.org/10.7461/jcen.2014.16.3.235
Abstract
OBJECTIVE
Several studies have reported on the effectiveness of fronto-lateral craniotomy in reducing the operating time and post-operative complications. However, no study has practically evaluated this method from the cosmetic point of view.
MATERIALS AND METHODS
We designed this study for comparison of the clinical differences and cosmetic outcomes between the frontolateral craniotomy and the conventional pterional craniotomy for clipping of unruptured intracranial aneurysms. We performed a retrospective analysis of the two groups based on their medical records and radiologic findings juxtaposed with their length of hospital stay, intensive care unit day and operation time, and the emergence of postoperative complication, mean size of aneurysm, and temporal depression.
RESULTS
After careful comparison of the thickness of temporalis muscle between the craniotomy side and the contralateral side, the results clearly showed that the conventional pterional craniotomy group was asymmetric by a p value of 0.152 and the frontolateral craniotomy group was symmetric by a p value of 0.002.
CONCLUSION
Frontolateral craniotomy could be a practical alternative for patients with an unruptured intracranial aneurysm in the anterior circulation including the posterior communicating artery, particularly those who are in a medically poor state or who highly demand minimal aesthetic mutilation.
Keyword
MeSH Terms
Figure
-
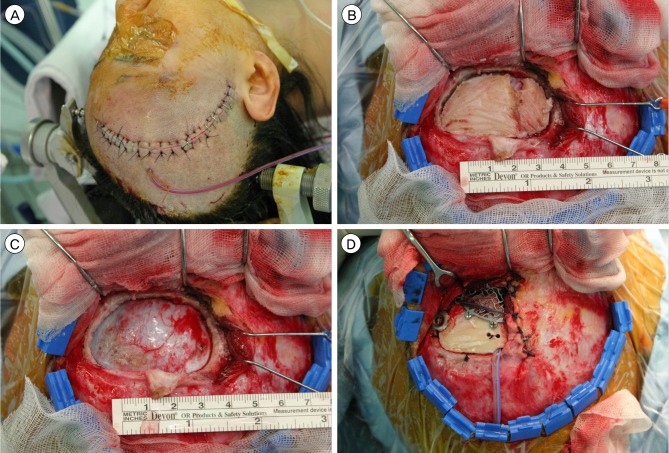
Fig. 1 (A) Minimal hair shaving was performed and the skin incision was short and was behind the hair line; (B) Only one burr hole is placed posteriorly just below the insertion line of the temporal muscle; (C) The mean size of the bone flap was 4×2.5 cm; (D) The temporal muscle is split only in its superior and anterior part. And in closure the bone flap was fixated with a skull fixator and a cranial plate.
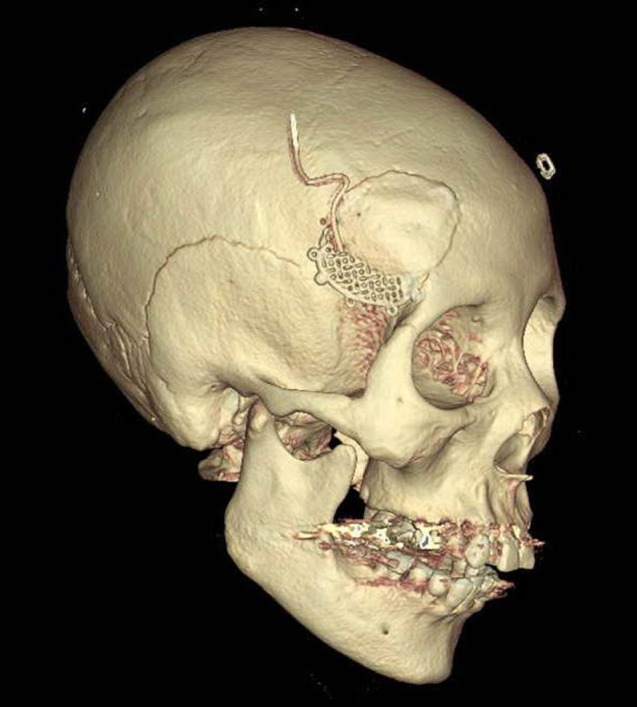
Fig. 2 The size of the craniotomy is absolutely sufficient to reach the whole anterior part of the circle of Willis, sellar, suprasellar legion and also the anterior part of the basilar artery if it is located superiorly from the posterior clinoid process.
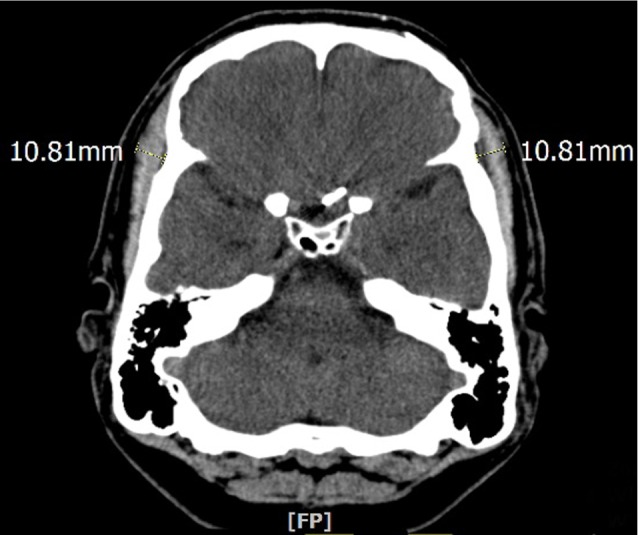
Fig. 3 Bilateral symmetry of temporalis muscle was measured through computed tomography taken six months after the operation.
Cited by 1 articles
-
Keyhole Approach and Neuroendoscopy for Cerebral Aneurysms
Won-Sang Cho, Jeong Eun Kim, Hyun-Seung Kang, Young-Je Son, Jae Seung Bang, Chang Wan Oh
J Korean Neurosurg Soc. 2017;60(3):275-281. doi: 10.3340/jkns.2017.0101.002.
Reference
-
1. Cha KC, Hong SC, Kim JS. Comparison between lateral supraorbital approach and pterional approach in the surgical treatment of unruptured intracranial aneurysms. J Korean Neurosurg Soc. 2012; 6. 51(6):334–337. PMID: 22949961.
Article2. Figueiredo EG, Deshmukh P, Nakaji P, Crusius MU, Crawford N, Spetzler RF, et al. The minipterional craniotomy: technical description and anatomic assessment. Neurosurgery. 2007; 11. 61(5 Suppl 2):256–264. discussion 264-65. PMID: 18091240.
Article3. Hernesniemi J, Ishii K, Niemela M, Smrcka M, Kivipelto L, Fujiki M, et al. Lateral supraorbital approach as an alternative to the classical pterional approach. Acta Neurochir Suppl. 2005; 94:17–21. PMID: 16060236.
Article4. Mori K, Yamamoto T, Nakao Y, Oyama K, Esaki T, Watanabe M, et al. Lateral supraorbital keyhole approach to clip unruptured anterior communicating artery aneurysms. Minim Invasive Neurosurg. 2008; 10. 51(5):292–297. PMID: 18855295.
Article5. Oikawa S, Mizuno M, Muraoka S, Kobayashi S. Retrograde dissection of the temporalis muscle preventing muscle atrophy for pterional craniotomy. Technical note. J Neurosurg. 1996; 2. 84(2):297–299. PMID: 8592239.6. Thompson N. Reconstructive Plastic Surgery. Philadelphia: WB Saunders;1977. p. 293–300.7. van Lindert E, Perneczky A, Fries G, Pierangeli E. The supraorbital keyhole approach to supratentorial aneurysms: concept and technique. Surg Neurol. 1998; 5. 49(5):481–489. discussion 489-90. PMID: 9586924.
Article8. Yasargil MG. Vertebrobasilar aneurysms. In : Yasargil MG, editor. Microneurosurgery. Stuttgart: Georg Thieme Verlag;1984. Vol 2:p. 232–295.9. Yasargil MG, Fox JL. The microsurgical approach to intracranial aneurysms. Surg Neurol. 1975; 1. 3(1):7–14. PMID: 1111150.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superciliary Keyhole Approach for Unruptured Anterior Circulation Aneurysms: Surgical Technique, Indications, and Contraindications
- Trans-supraorbital Approach to Anterior Circulation Aneurysms
- Minimally Invasive and Tailored Surgical Approach to the Anterior Circulation Aneurysms
- Superior Orbital Rim Approach to the Anterior Circulation Aneurysms: Surgical Technique
- Unruptured Supraclinoid Internal Carotid Artery Aneurysm Surgery : Superciliary Keyhole Approach versus Pterional Approach
