The Outcomes of Treatment for Sacrococcygeal Teratoma: The 24-year Experiences
- Affiliations
-
- 1Pediatric Surgery, University of Ulsan College of Medicine and Asan Medical Center, Seoul, Korea. sckim@amc.seoul.kr
- 2Department of Surgery, University of Ulsan College of Medicine and GangNeung Asan Medical Center, GangNeung, Korea.
- 3Department of Pathology, University of Ulsan College of Medicine and Asan Medical Center, Seoul, Korea.
- KMID: 1961498
- DOI: http://doi.org/10.13029/jkaps.2013.19.2.81
Abstract
- The purposes of this study was to describe the clinical correlation of mass size and gestational age, prognostic factors in sacrococcygeal teratoma (SCT) at a tertiary pediatric surgery, University of Ulsan College of Medicine and Asan Medical Center (AMC), Seoul, Korea. Fifty five patients admitted to the AMC with a SCT between May 1989 and April 2013 were included in this retrospective review. Mean follow up was 861 days. Mean maternal age at delivery was 30 +/- 2.7 year, mean gestational age (GA) was 36.9 +/- 3.6wks, and preterm delivery was 21.8%. Birth body weight was 3182 +/- 644 g and male vs. female ratio was 1:2.05. We can't find significant difference between Caesarean section and maternal age at delivery (p = 0.817). But, caesarean section was favored by gestational age (p = 0.002), larger tumor size (p = 0.029) or higher tumor weight fraction rate to birth body weight (p = 0.024). Type I was 13, II 21, III 17, and IV 3 according to Altman et al. classification. The tumor component was predominantly cystic(>50%) in 73.1%. And the majority histological classification of tumors were mature teratoma (70.3%). The motality rate was 5.5%. Three patients expired because of postpartum bleeding, post-op bleeding related complication such as DIC. SCT recurred in four patients. The interval between first and second operation was 206.2 +/- 111.0 d (range 53~325 d). In two patients, serum AFP levels were elevated at a regular checkup without any symptom, and subsequent imaging studies revealed SCT. The most common cause of death was bleeding and bleeding related complication. So Caesarean section and active peripartum and perioperative management will be needed for huge solid SCT. In the case of Yolk sac tumor or huge immature teratoma, possibility of recurrence have to be always considered, so follow up by serial AFP and MRI is important for SCT management.
Keyword
MeSH Terms
-
Body Weight
Cause of Death
Cesarean Section
Chungcheongnam-do
Classification
Dacarbazine
Endodermal Sinus Tumor
Female
Follow-Up Studies
Gestational Age
Hemorrhage
Humans
Korea
Magnetic Resonance Imaging
Male
Maternal Age
Parturition
Peripartum Period
Postpartum Period
Pregnancy
Recurrence
Retrospective Studies
Seoul
Teratoma*
Tumor Burden
Dacarbazine
Figure
-
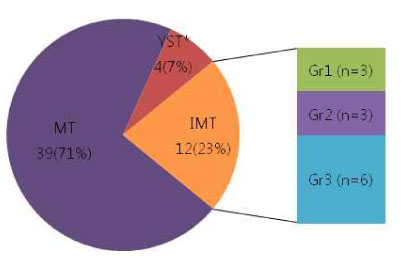
Fig. 1 Histological classification MT; Mature teratoma, IMT; Immature teratoma, YST; York sac tumor, Gr;Grade * Three patients with mixed type consisting of YST and mature and immature teratoma are included in this group
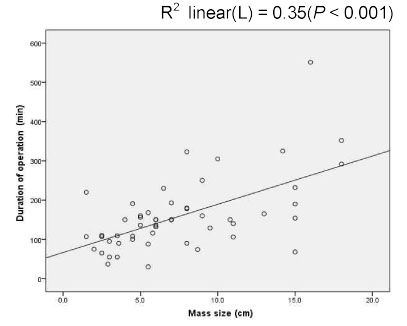
Fig. 2 Duration of operation and Mass size by univariate linear regression analyses
Cited by 1 articles
-
Sacrococcygeal Teratoma: A Survey by the Korean Association of Pediatric Surgeons in 2018
Jung-Tak Oh, Hye Kyung Chang, Min Jeong Cho, Yong Hoon Cho, Soo Jin Na Choi, Yoon Mi Choi, Jae Hee Chung, Sang Young Chung, Jeong Hong, Seok Joo Han, Yeon Jun Jeong, Eunyoung Jung, Kyuhwan Jung, Dae Youn Kim, Hae-Young Kim, Hyun-Young Kim, Ki Hoon Kim, Sang Youn Kim, Seong Chul Kim, Seong Min Kim, Soo-Hong Kim, Jong-In Lee, Myung-Duk Lee, Nam-Hyuk Lee, Suk-Koo Lee, So Hyun Nam, Jin Young Park, Kwi-Won Park, Tae-Jin Park, Jeong-Meen Seo, Jae Ho Shin, Jiyoung Sul
Adv Pediatr Surg. 2019;25(2):35-43. doi: 10.13029/aps.2019.25.2.35.
Reference
-
1. Usui N, Kitano Y, Sago H, et al. Outcomes of prenatally diagnosed sacrococcygeal teratomas: the results of a Japanese nationwide survey. J Pediatr Surg. 2012; 47(3):441–447.2. Altman RP, Randolph JG, Lilly JR. Sacrococcygeal teratoma: American Academy of Pediatrics Surgical Section Survey-1973. J Pediatr Surg. 1974; 9(3):389–398.3. Ho KO, Soundappan SV, Walker K, Badawi N. Sacrococcygeal teratoma: the 13-year experience of a tertiary paediatric centre. J Paediatr Child Health. 2011; 47(5):287–291.4. Isaacs H Jr. Perinatal (fetal and neonatal) germ cell tumors. J Pediatr Surg. 2004; 39(7):1003–1013.5. Swamy R, Embleton N, Hale J. Sacrococcygeal teratoma over two decades: Birth prevalence, prenatal diagnosis and clinical outcomes. Prenatal Diagnosis. 2008; 28(11):1048–1051.6. Dewan PA, Davidson PM, Campbell PE, Tiedemann K, Jones PG. Sacrococcygeal teratoma: has chemotherapy improved survival? J Pediatr Surg. 1987; 22(3):274–277.7. Bilik R, Shandling B, Pope M, Thorner P, Weitzman S, Ein SH. Malignant benign neonatal sacrococcygeal teratoma. J Pediatr Surg. 1993; 28(9):1158–1160.8. Huddart SN, Mann JR, Robinson K, et al. Sacrococcygeal teratomas: the UK Childre's Cancer Study Group's experience. I. Neonatal. Pediatr Surg Int. 2003; 19(1-2):47–51.9. Gabra HO, Jesudason EC, McDowell HP, Pizer BL, Losty PD. Sacrococcygeal teratoma-a 25-year experience in a UK regional center. J Pediatr Surg. 2006; 41(9):1513–1516.10. Graf JL, Albanese CT. Fetal Sacrococcygeal Teratoma. World J Surg. 2003; 27(1):84–86.11. Sy ED, Filly RA, Cheong M-L, et al. Prognostic Role of Tumor-Head Volume Ratio in Fetal Sacrococcygeal Teratoma. Fetal Diagnosis and Therapy. 2009; 26(2):75–80.12. Coleman A, Kline-Fath B, Keswani S, Lim F-Y. Prenatal solid tumor volume index: novel prenatal predictor of adverse outcome in sacrococcygeal teratoma. J Surg Res. 2013; 184(1):330–336.13. Shue E, Bolouri M, Jelin EB, et al. Tumor metrics and morphology predict poor prognosis in prenatally diagnosed sacrococcygeal teratoma: A 25-year experience at a single institution. J Pediatr Surg. 2013; 48(6):1225–1231.14. Labdenne P, Heikinheimo M. Clinical use of tumor markers in childhood malignancies. Ann Med. 2002; 34(5):316–323.15. Rescorla FJ, Sawin RS, Coran AG, Dillon PW, Azizkhan RG. Long-term outcome for infants and children with sacrococcygeal teratoma: a report from the Childrens Cancer Group. J Pediatr Surg. 1998; 33(2):171–176.16. Yoshida M, Matsuoka K, Nakazawa A, et al. Sacrococcygeal yolk sac tumor developing after teratoma: A clinicopathological study of pediatric sacrococcygeal germ cell tumors and a proposal of the pathogenesis of sacrococcygeal yolk sac tumors. J Pediatr Surg. 2013; 48(4):776–781.
