J Korean Assoc Oral Maxillofac Surg.
2014 Feb;40(1):11-16. 10.5125/jkaoms.2014.40.1.11.
Three-dimensional evaluation of lingual split line after bilateral sagittal split osteotomy in asymmetric prognathism
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Pusan National University, Yangsan, Korea. ydkimdds@pusan.ac.kr
- KMID: 1960966
- DOI: http://doi.org/10.5125/jkaoms.2014.40.1.11
Abstract
OBJECTIVES
The aim of this study was to evaluate the pattern of lingual split line when performing a bilateral sagittal split osteotomy (BSSO) for asymmetric prognathism. This was accomplished with the use of cone-beam computed tomography (CBCT) and three-dimensional (3D) software program.
MATERIALS AND METHODS
The study group was comprised of 40 patients (20 males and 20 females) with asymmetric prognathism, who underwent BSSO (80 splits; n=80) from January 2012 through June 2013. We observed the pattern of lingual split line using CBCT data and image analysis program. The deviated side was compared to the contralateral side in each patient. To analyze the contributing factors to the split pattern, we observed the position of the lateral cortical bone cut end and measured the thickness of the ramus that surrounds the mandibular lingula.
RESULTS
The lingual split patterns were classified into. The true "Hunsuck" line was 60.00% (n=48), and the bad split was 7.50% (n=6). Ramal thickness surrounding the lingual was 5.55+/-1.07 mm (deviated) and 5.66+/-1.34 mm (contralateral) (P=0.409). The position of the lateral cortical bone cut end was classified into three types: A, lingual; B, inferior; C, buccal. Type A comprised 66.25% (n=53), Type B comprised 22.50% (n=18), and Type C comprised 11.25% (n=9).
CONCLUSION
In asymmetric prognathism patients, there were no differences in the ramal thickness between the deviated side and the contralateral side. Furthermore, no differences were found in the lingual split pattern. The lingual split pattern correlated with the position of the lateral cortical bone cut end. In addition, the 3D-CT reformation was a useful tool for evaluating the surgical results of BSSO of the mandible.
MeSH Terms
Figure
-

Fig. 1 Orientation of three-dimensional images and measurement point. A, B. Reference plane and orientation. C. Level of measurement at the mandibular lingual. D. Measurement of ramal thickness.
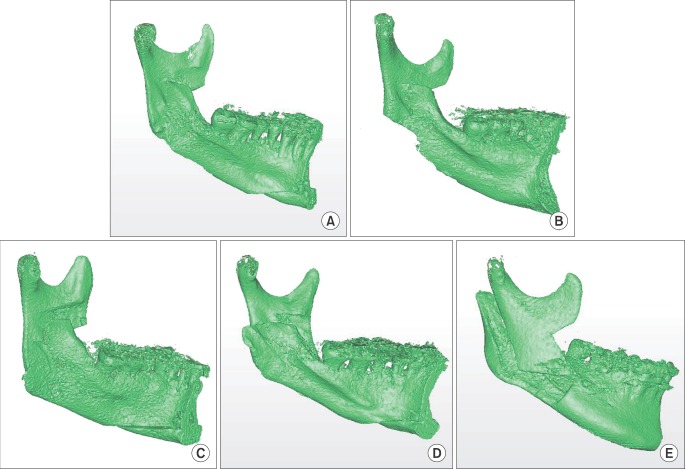
Fig. 2 The five types of lingual split pattern. A. Type I. B. Type II. C. Type III. D. Type IV. E. Type V.
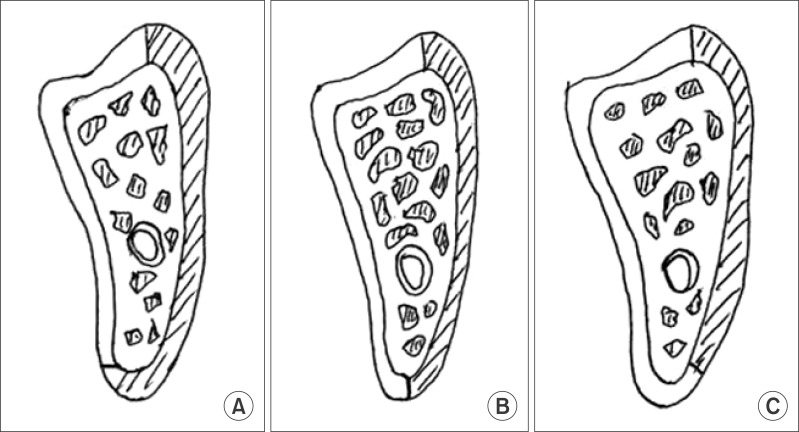
Fig. 3 Position of the lateral cortical bone end. A. Lingual. B. Inferior. C. Buccal.
Reference
-
1. Trauner R, Obwegeser H. The surgical correction of mandibular prognathism and retrognathia with consideration of genioplasty. I. Surgical procedures to correct mandibular prognathism and reshaping of the chin. Oral Surg Oral Med Oral Pathol. 1957; 10:677–689. PMID: 13441284.2. Dal Pont G. Retromolar osteotomy for the correction of prognathism. J Oral Surg Anesth Hosp Dent Serv. 1961; 19:42–47. PMID: 13719390.3. Hunsuck EE. A modified intraoral sagittal splitting technic for correction of mandibular prognathism. J Oral Surg. 1968; 26:250–253. PMID: 5237786.4. Plooij JM, Naphausen MT, Maal TJ, Xi T, Rangel FA, Swennnen G, et al. 3D evaluation of the lingual fracture line after a bilateral sagittal split osteotomy of the mandible. Int J Oral Maxillofac Surg. 2009; 38:1244–1249. PMID: 19713076.
Article5. Muto T, Takahashi M, Akizuki K. Evaluation of the mandibular ramus fracture line after sagittal split ramus osteotomy using 3-dimensional computed tomography. J Oral Maxillofac Surg. 2012; 70:e648–e652. PMID: 23078827.
Article6. Baek SH, Cho IS, Chang YI, Kim MJ. Skeletodental factors affecting chin point deviation in female patients with class III malocclusion and facial asymmetry: a three-dimensional analysis using computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 104:628–639. PMID: 17656131.
Article7. You KH, Lee KJ, Lee SH, Baik HS. Three-dimensional computed tomography analysis of mandibular morphology in patients with facial asymmetry and mandibular prognathism. Am J Orthod Dentofacial Orthop. 2010; 138:540.e1–540.e8. PMID: 21055584.
Article8. Klinge B, Petersson A, Maly P. Location of the mandibular canal: comparison of macroscopic findings, conventional radiography, and computed tomography. Int J Oral Maxillofac Implants. 1989; 4:327–332. PMID: 2639861.9. Kondo T, Ong SH, Foong KW. Computer-based extraction of the inferior alveolar nerve canal in 3-D space. Comput Methods Programs Biomed. 2004; 76:181–191. PMID: 15501505.
Article10. Yang WS. The study on the orthodontic patients who visited department of orthodontics, Seoul National University Hospital during 10 years (1985-1994). Korean J Orthod. 1995; 25:497–509.11. Yoon KS, Jung YS, Kang GC, Park HS. Facial asymmetry with mandibular prognathism: a new trial of classification and interpretation. J Korean Assoc Oral Maxillofac Surg. 2004; 30:108–120.12. Kwon TG, Park HS, Ryoo HM, Lee SH. A comparison of craniofacial morphology in patients with and without facial asymmetry--a three-dimensional analysis with computed tomography. Int J Oral Maxillofac Surg. 2006; 35:43–48. PMID: 15925488.
Article13. Kwon TG, Lee KH, Park HS, Ryoo HM, Kim HJ, Lee SH. Relationship between the masticatory muscles and mandibular skeleton in mandibular prognathism with and without asymmetry. J Oral Maxillofac Surg. 2007; 65:1538–1543. PMID: 17656280.
Article14. Yamamoto R, Nakamura A, Ohno K, Michi KI. Relationship of the mandibular canal to the lateral cortex of the mandibular ramus as a factor in the development of neurosensory disturbance after bilateral sagittal split osteotomy. J Oral Maxillofac Surg. 2002; 60:490–495. PMID: 11988921.
Article15. Lee JY, Kim YI, Hwang DS, Kim YD, Shin SH, Kim UK, et al. Cross-sectional study of the mandibular body in patients with facial asymmetry. J Korean Assoc Oral Maxillofac Surg. 2011; 37:109–113.
Article16. Wolford LM, Davis WM Jr. The mandibular inferior border split: a modification in the sagittal split osteotomy. J Oral Maxillofac Surg. 1990; 48:92–94. PMID: 2294218.
Article17. MacIntosh RB. Experience with the sagittal osteotomy of the mandibular ramus: a 13-year review. J Maxillofac Surg. 1981; 9:151–165. PMID: 6974211.
Article18. Turvey TA. Intraoperative complications of sagittal osteotomy of the mandibular ramus: incidence and management. J Oral Maxillofac Surg. 1985; 43:504–509. PMID: 3859593.
Article19. Panula K, Finne K, Oikarinen K. Incidence of complications and problems related to orthognathic surgery: a review of 655 patients. J Oral Maxillofac Surg. 2001; 59:1128–1136. PMID: 11573165.
Article20. Guernsey LH, DeChamplain RW. Sequelae and complications of the intraoral sagittal osteotomy in the mandibular rami. Oral Surg Oral Med Oral Pathol. 1971; 32:176–192. PMID: 5284103.
Article21. Veras RB, Kriwalsky MS, Hoffmann S, Maurer P, Schubert J. Functional and radiographic long-term results after bad split in orthognathic surgery. Int J Oral Maxillofac Surg. 2008; 37:606–611. PMID: 18515045.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stability after Surgical Correction of Mandibular Prognathism Using Bilateral Sagittal Split Ramus Osteotomy with Rigid Fixation
- Facial nerve palsy after sagittal split ramus osteotomy in severe mandibular prognathism: a case report
- Analysis of short face tendency and it's determinant factors after bilateral sagittal split ramus osteotomy of mandibular prognathism
- Stability of unilateral sagittal split ramus osteotomy for correction of facial asymmetry: long-term case series and literature review
- A clinical study on the effects of bilateral sagittal split ramus osteotomy on the postoperative condylar positional changes in the mandibular prognathism
