Indirect Decompression using Segmental Screw Fixation for Cervical Myelopathy Caused by C1-2 Subluxation: Technical Note
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul Medical Center, Seoul, Korea.
- 2Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. ortho@hananet.net
- KMID: 1947790
- DOI: http://doi.org/10.4055/jkoa.2007.42.6.815
Abstract
- The main aims of surgery for severe cord compression and myelopathy caused by atlantoaxial subluxation are decompression of the spinal cord and achievement of rigid fixation and fusion. Direct decompression by resecting the bony structures that compress the spinal cord includes transoral decompression and resection of the posterior arch of the atlas. The shortcomings of these procedures are a high complication rate and a relatively low rate of union. Indirect decompression can be performed by a reduction of the subluxation and fixation without bone resection. To the best of our knowledge, there are no domestic reports on the use of indirect decompression for severe cord compression and myelopathy for atlantoaxial subluxation. We report a case of a patient that had atlantoaxial subluxation and severe myelopathy; satisfactory reduction of the subluxation and decompression with an improvement in the myelopathy symptoms was achieved by indirect decompression using segmental screw fixation.
Keyword
Figure
-
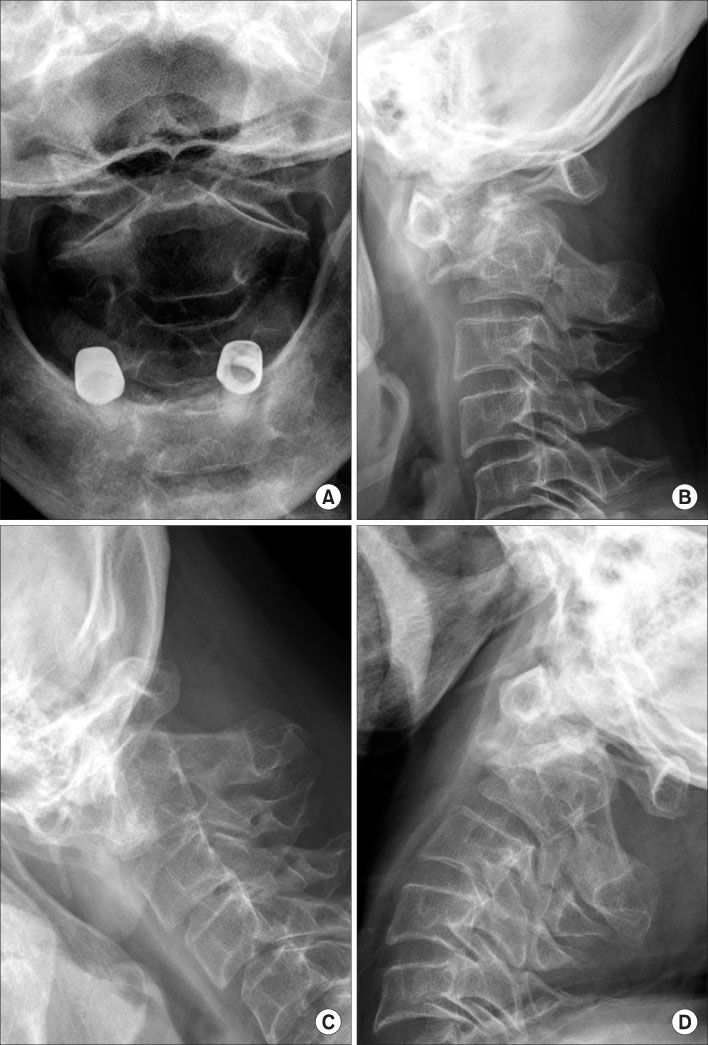
Fig. 1 Preoperative radiographs are shown. Open mouth anteroposterior (A) and lateral (B) radiographs taken in neutral position show severe subluxation of the atlantoaxial joint. Lateral radiographs in flexion (C) and extension (D) show only minimal motion in the atlantoaxial joint.
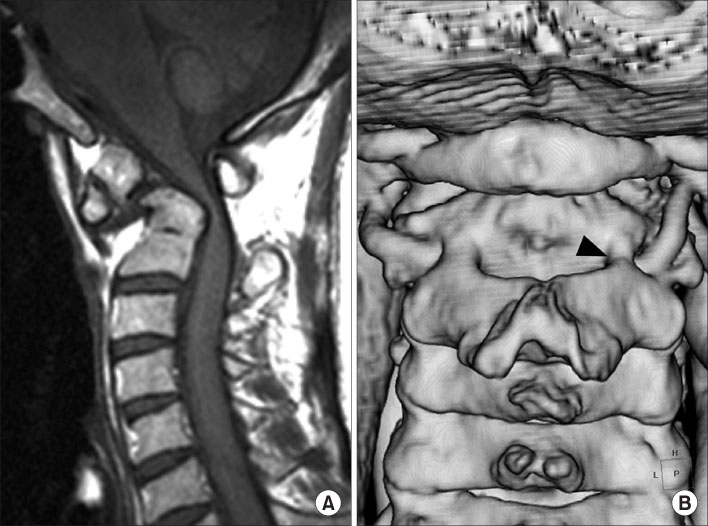
Fig. 2 Preoperative MRI and CT-angiography are shown. (A) MRI shows severe compression of the spinal cord. (B) CT-angiography shows that the pedicles are too small for screw insertion, particularly on the right side (arrowhead).
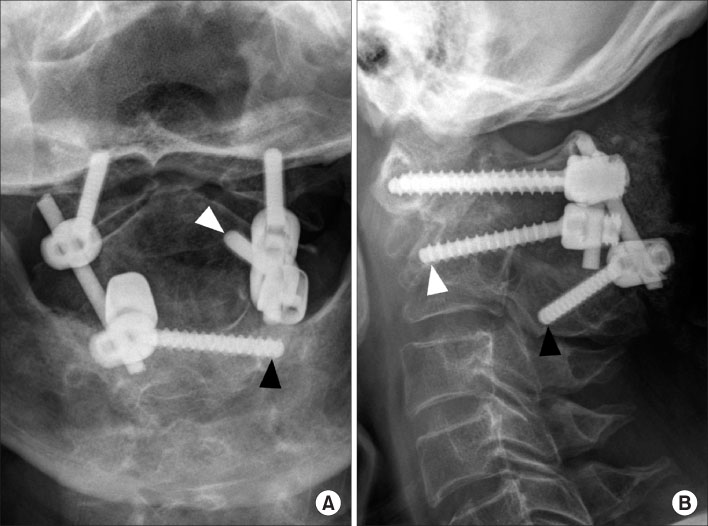
Fig. 3 Radiographs taken 3 months after surgery are shown. A subarticualr screw on the left side (white arrowheads) and a laminar screw inserted from the right side (black arrowheads) of C2 are shown.
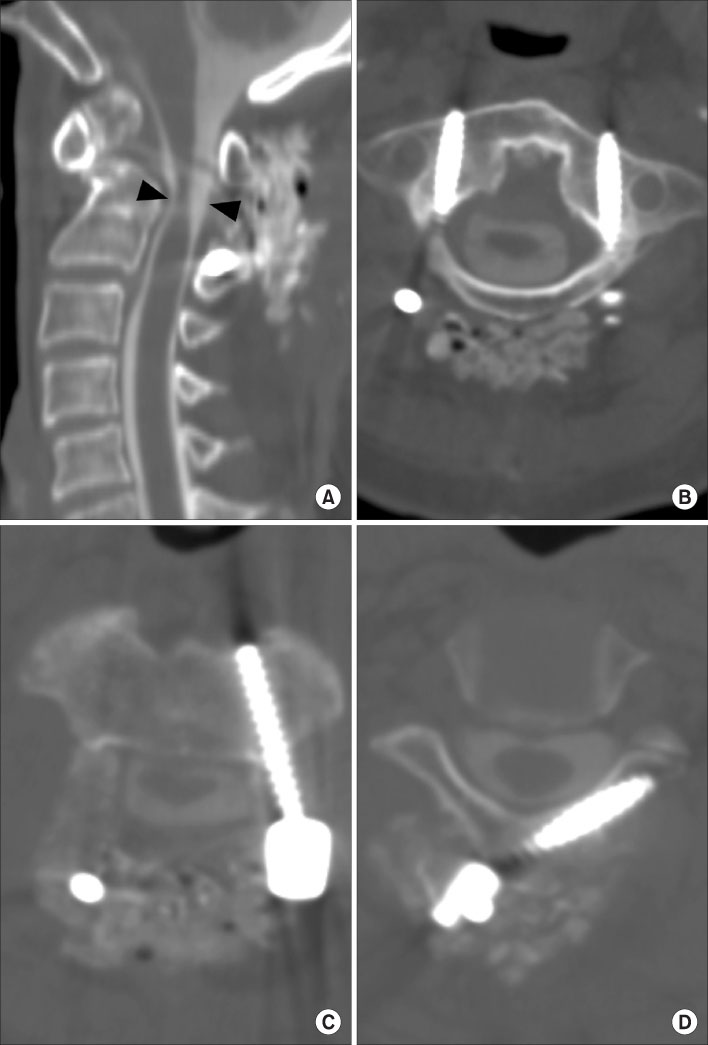
Fig. 4 CT-myelogram images taken 4 days after surgery are shown. (A) A sagittal reconstruction image shows satisfactory reduction and decompression of the spinal cord. Although the atrophic spinal cord is not fully expanded, the thecal sac is well expanded (arrowheads). (B) C1 lateral mass screws are placed bicortically in a good position. (C) A subarticular screw is shown on the left side of C2. (D) A laminar screw placed from the right side of C2 is shown.
Reference
-
1. Bonney G, Williams JP. Trans-oral approach to the upper cervical spine. A report of 16 cases. J Bone Joint Surg Br. 1985. 67:691–698.
Article2. Fang HSY, Ong GB. Direct anterior approach to the upper cervical spine. J Bone Joint Surg Am. 1962. 44:1588–1604.
Article3. Goel A, Desai KI, Muzumdar DP. Atlantoaxial fixation using plate and screw method: a report of 160 treated patients. Neurosurgery. 2002. 51:1351–1357.
Article4. Harms J, Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine. 2001. 26:2467–2471.
Article5. Kim KH, Yeom JS, Park KW, Hong SW, Chang BS, Lee CK. Old atlantoaxial rotary subluxation associated with high-riding vertebral arteries: arthrodesis using C1 lateral mass screws and C2 laminar screws: a case of report. J Korean Fracture Soc. 2007. 20:90–93.6. Nagashima C. Surgical treatment of irreducible atlanto-axial dislocation with spinal cord compression. Case report. J Neurosurg. 1973. 38:374–378.7. Stanley D, Laing RJ, Forster DM, Getty CJ. Posterior decompression and fusion in rheumatoid disease of the cervical spine: redressing the balance. J Spinal Disord. 1994. 7:439–443.8. Subin B, Liu JF, Marshall GJ, Huang HY, Ou JH, Xu GZ. Transoral anterior decompression and fusion of chronic irreducible atlantoaxial dislocation with spinal cord compression. Spine. 1995. 20:1233–1240.
Article9. Wright NM. Posterior C2 fixation using bilateral, crossing C2 laminar screws: case series and technical note. J Spinal Disord Tech. 2004. 17:158–162.10. Yeom JS, Won JH, Park SK, et al. The subarticular screw: a new trajectory for the C2 screw. J Korean Soc Spine Surg. 2006. 13:75–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atlantoaxial Fixation using C2 Subarticular Screws and C1 Lateral Mass Screws : A Technical Report
- Old Atlantoaxial Rotary Subluxation Associated with High-riding Vertebral Arteries: Arthrodesis Using C1 Lateral Mass Screws and C2 Laminar Screws: A Case Report
- Application of C1-C3 Halifax Interlaminar Clamps in Addition to C1-C2 Cable Fixation
- Atlantoaxial Subluxation due to Psoriatic Arthritis
- Posterior C1-2 Transarticular Screw Fixation in Atlantoaxial Instability
