Well-Differentiated Pancreatic Neuroendocrine Tumor with Solitary Hepatic Metastasis Presenting as a Benign Cystic Mass: A Case Report
- Affiliations
-
- 1Department of Radiology, Gachon University Gil Hospital, Incheon, Korea. sjchoi@gilhospital.com
- KMID: 1941780
- DOI: http://doi.org/10.3348/jksr.2014.70.5.351
Abstract
- Pancreatic neuroendocrine tumors and their hepatic metastases have an inconsistent appearance with only a small percentage of lesions appearing as cystic masses in computed tomography (CT) and magnetic resonance imaging (MRI). Therefore, they can be mistaken as benign or infectious lesions, which can lead to a false diagnosis with delayed or inadequate treatment. We reported a patient with upper abdominal pain that lasted for several months, caused by a huge cystic neuroendocrine carcinoma of the liver. This was mistakenly interpreted as a complicated or hydatid cyst, and the findings in the CT and MRI was presented.
MeSH Terms
Figure
-
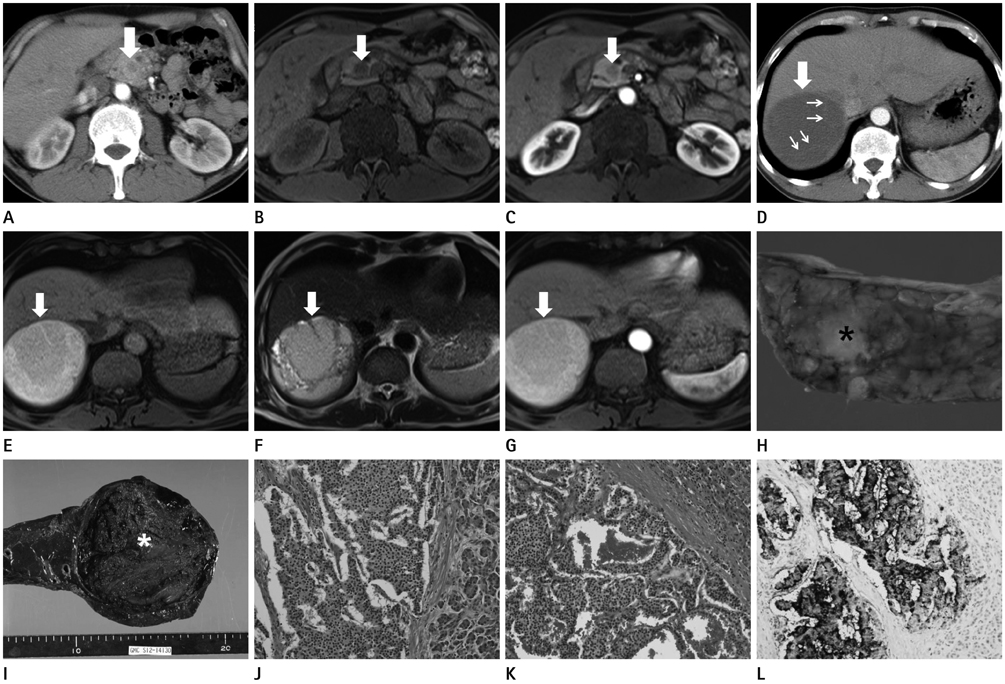
Fig. 1 A 50-year-old man presented with a week's history of epigastric pain. A. Transverse CT scan shows a 15 mm hypodense mass in head of pancreas compared with the normal pancreas parenchyma (arrow). B. T1-weighted MR image shows a 15 mm hypointense mass in head of pancreas compared with the normal pancreas parenchyma (arrow). C. T1-weighted image after application of Gd-EOB-DTPA shows subtle enhancement of the mass in the arterial phase (arrow). D. Transverse CT scan shows a 10 cm hypodense mass (thick arrow) in the right hepatic lobe with suspicious internal thin septa (thin arrows). E. T1-weighted MR image shows a 10 cm hyperintense mass in the right hepatic lobe with suspicious internal thin septa (arrow). F. T2-weighted MR image shows hyperintense mass including internal multiple septations (arrow). G. On T1-weighted image after contrast media injection, no Gd-EOB-DTPA uptake of the mass is present (arrow). H. A photograph of the resected pancreatic specimen shows the 23 mm irregular margined yellowish mass (asterisk) in head of pancreas. I. A photograph of the resected hepatic specimen shows the large liver mass (asterisk) possessing a capsule, containing hemorrhages. J. Histology of the neuroendocrine carcinoma in the pancreas. Tumor cells featuring abundant cytoplasm, prominent nucleoli; frequent mitotic rate shows the organoid, nesting, trabecular and palisading pattern (H&E, × 200). K, L. Histology of the neuroendocrine carcinoma in the liver. Tumor cells featuring abundant cytoplasm, prominent nucleoli; frequent mitotic rate shows the organoid, nesting, trabecular and palisading pattern (H&E, × 200) (K). Positive immunohistochemical stain for synaptophysin (synaptophysin, × 200) (L).
Reference
-
1. Gumbs AA, Moore PS, Falconi M, Bassi C, Beghelli S, Modlin I, et al. Review of the clinical, histological, and molecular aspects of pancreatic endocrine neoplasms. J Surg Oncol. 2002; 81:45–53. discussion 54.2. Franko J, Feng W, Yip L, Genovese E, Moser AJ. Non-functional neuroendocrine carcinoma of the pancreas: incidence, tumor biology, and outcomes in 2,158 patients. J Gastrointest Surg. 2010; 14:541–548.3. Bosman FT, Cameiro F, Hruban RH. WHO Classification of Tumours of the Digestive System. 4th ed. Lyon: International Agency for Research on Cancer (IARC);2010. p. 13–14. p. 64–68.4. O'Toole D, Ruszniewski P. Chemoembolization and other ablative therapies for liver metastases of gastrointestinal endocrine tumours. Best Pract Res Clin Gastroenterol. 2005; 19:585–594.5. Oberg K, Eriksson B. Endocrine tumours of the pancreas. Best Pract Res Clin Gastroenterol. 2005; 19:753–781.6. Sarmiento JM, Farnell MB, Que FG, Nagorney DM. Pancreaticoduodenectomy for islet cell tumors of the head of the pancreas: long-term survival analysis. World J Surg. 2002; 26:1267–1271.7. Debray MP, Geoffroy O, Laissy JP, Lebtahi R, Silbermann-Hoffman O, Henry-Feugeas MC, et al. Imaging appearances of metastases from neuroendocrine tumours of the pancreas. Br J Radiol. 2001; 74:1065–1070.8. Krohn M, Grieser C, Weichert W, Pascher A, Denecke T. Well-differentiated neuroendocrine carcinoma mimicking an echinococcus cyst of the liver in CT-MRI findings with hepatocyte specific contrast material. J Gastrointestin Liver Dis. 2011; 20:439–442.9. Musunuru S, Chen H, Rajpal S, Stephani N, McDermott JC, Holen K, et al. Metastatic neuroendocrine hepatic tumors: resection improves survival. Arch Surg. 2006; 141:1000–1004. discussion 1005.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Gastric Neuroendocrine Tumor with Hepatic Metastasis
- Pancreatic Collision Tumor of Desmoid-Type Fibromatosis and Mucinous Cystic Neoplasm: A Case Report
- Long-term Survival in Patient with Metastatic Pancreatic Neuroendocrine Tumor Treated by Variable Treatment
- Surgical Results of Pancreatic Neuroendocrine Tumors
- Case report of solitary giant hepatic lymphangioma
