Persistent Aneurysm Growth Following Pipeline Embolization Device Assisted Coiling of a Fusiform Vertebral Artery Aneurysm: A Word of Caution!
- Affiliations
-
- 1Department of Neurosurgery, Rush University Medical Center, Chicago, U.S.A. Manish_Kasliwal@rush.edu
- KMID: 1910757
- DOI: http://doi.org/10.5469/neuroint.2015.10.1.28
Abstract
- The complex morphology of vertebrobasilar fusiform aneurysms makes them one of the most challenging lesions treated by neurointerventionists. Different management strategies in the past included parent vessel occlusion with or without extra-intracranial bypass surgery and endovascular reconstruction by conventional stents. Use of flow diversion has emerged as a promising alternative option with various studies documenting its efficacy and safety. However, there are various caveats associated with use of flow diversion in patients with fusiform vertibrobasilar aneurysms especially in patients presenting with acute subarachnoid hemorrhage (SAH). We report a rare case of persistent aneurysmal growth after coiling and placement of the Pipeline Embolization Device (PED; ev3, Irvine, California, USA) for SAH from a fusiform vertebral artery aneurysm. As consequences of aneurysm rupture can be devastating especially in patients with a prior SAH, the clinical relevance of recognizing and understanding such patterns of failure cannot be overemphasized as highlighted in the present case.
Keyword
MeSH Terms
Figure
-
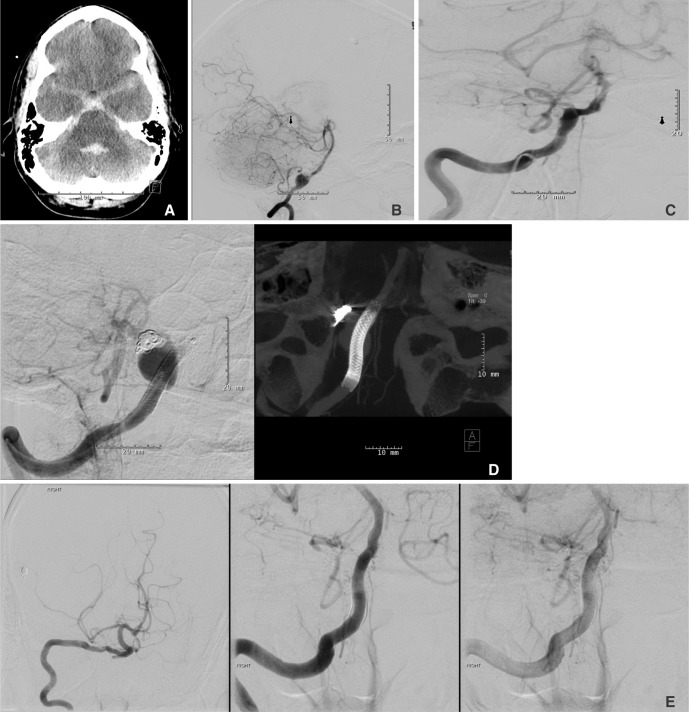
Fig. 1 A. Axial computed tomography (CT) scan of the head showing presence of Fisher grade 3 SAH. B. Digital subtraction angiography (DSA) demonstrating right vertebral artery fusiform aneurysm with the PICA takeoff arising from the base of a focal dilatation from the fusiform aneurysm segment. C. Post embolization DSA showing deployment of a 3.75 × 18 mm PED completely covering the fusiform vertebral aneurysm along with Raymond class II occlusion of the focal dilatation arising from the fusiform aneurysm. D. Follow up angiogram at 6 months showing the presence of aneurysm regrowth and coil compaction (left panel) despite well deployed PED across the aneurysm (right panel). E. Anteroposterior (left panel) and lateral (middle and right panels) images from DSA performed 3 months after the second procedure showing remodeling of the right vertebral artery with no residual or recurrent aneurysm.
Reference
-
1. Wang Q, Leng B, Song D, Chen G. Fusiform aneurysms of the vertebrobasilar arterial trunk: choice of endovascular methods and therapeutic efficacy. Acta Neurochir (Wien). 2010; 152:1467–1476. PMID: 20496084.
Article2. Tan LA, Keigher KM, Munich SA, Moftakhar R, Lopes DK. Thromboembolic complications with Pipeline Embolization Device placement: impact of procedure time, number of stents and pre-procedure P2Y12 reaction unit (PRU) value. J Neurointerv Surg. 2015; 7:217–221. PMID: 24553344.
Article3. Becske T, Kallmes DF, Saatci I, McDougall CG, Szikora I, Lanzino G, et al. Pipeline for uncoilable or failed aneurysms: results from a multicenter clinical trial. Radiology. 2013; 267:858–868. PMID: 23418004.
Article4. Cruz JP, O'Kelly C, Kelly M, Wong JH, Alshaya W, Martin A, et al. Pipeline embolization device in aneurysmal subarachnoid hemorrhage. AJNR Am J Neuroradiol. 2013; 34:271–276. PMID: 23064594.
Article5. Pistocchi S, Blanc R, Bartolini B, Piotin M. Flow diverters at and beyond the level of the circle of willis for the treatment of intracranial aneurysms. Stroke. 2012; 43:1032–1038. PMID: 22282890.
Article6. Chung J, Lim YC, Suh SH, Shim YS, Kim YB, Joo JY, et al. Stent-assisted coil embolization of ruptured wide-necked aneurysms in the acute period: incidence of and risk factors for periprocedural complications. J Neurosurg. 2014; 121:4–11. PMID: 24834945.
Article7. Martin AR, Cruz JP, Matouk CC, Spears J, Marotta TR. The pipeline flow-diverting stent for exclusion of ruptured intracranial aneurysms with difficult morphologies. Neurosurgery. 2012; 70(1 Suppl Operative):21–28. PMID: 21841519.
Article8. Chalouhi N, Tjoumakaris SI, Gonzalez LF, Hasan D, Pema PJ, Gould G, et al. Spontaneous delayed migration/shortening of the pipeline embolization device: report of 5 cases. AJNR Am J Neuroradiol. 2013; 34:2326–2330. PMID: 23811979.
Article9. Lylyk P, Miranda C, Ceratto R, Ferrario A, Scrivano E, Luna HR, et al. Curative endovascular reconstruction of cerebral aneurysms with the pipeline embolization device: the Buenos Aires experience. Neurosurgery. 2009; 64:632–642. PMID: 19349825.10. Jabbour P, Chalouhi N, Tjoumakaris S, Gonzalez LF, Dumont AS, Randazzo C, et al. The Pipeline Embolization Device: learning curve and predictors of complications and aneurysm obliteration. Neurosurgery. 2013; 73:113–120. PMID: 23615106.11. Fischer S, Perez MA, Kurre W, Albes G, Bazner H, Henkes H. Pipeline embolization device for the treatment of intra- and extracranial fusiform and dissecting aneurysms: initial experience and long-term follow-up. Neurosurgery. 2014; 75:364–374. PMID: 24871140.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment for Giant Fusiform Aneurysm Located in the Cavernous Segment of the Internal Carotid Artery Using the Pipeline Embolization Device
- Inadvertent Complication of a Pipeline Embolization Device for Treatment with Vertebral Artery Dissecting Aneurysm : Distal Tip Fracture of Delivery Wire
- Dual Stent-Assisted Coil Embolization for Fusiform Aneurysm Arising From Persistent Trigeminal Artery
- Treatment of a Ruptured Vertebrobasilar Fusiform Aneurysm Using Pipeline Embolization Device
- A Case of Migration of Pipeline Embolization Device Causing Rupture during Treatment of an Unruptured Vertebral Artery Dissecting Aneurysm
