Role of resection for Bismuth type IV hilar cholangiocarcinoma and analysis of determining factors for curative resection
- Affiliations
-
- 1Department of Surgery, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, Goyang, Korea.
- 2Department of Surgery and Cancer Research Institute, Seoul National University College of Medicine, Seoul, Korea. jangjy4@snu.ac.kr
- KMID: 1882836
- DOI: http://doi.org/10.4174/astr.2014.87.2.87
Abstract
- PURPOSE
Extended liver resection may provide long-term survival in selected patients with Bismuth type IV hilar cholangiocarcinoma (HCCA). The purpose of this study was to identify anatomical factors that predict curative-intended resection.
METHODS
Thirty-three of 159 patients with Bismuth type IV HCCA underwent major hepato-biliary resection with curative intent (CIR) between 2000 and 2010. Disease extent and anatomical variations were analyzed as factors enabling CIR.
RESULTS
CIR ratio with hilar trifurcation bile duct variation (13/16) was significantly higher than that with other bile duct variation types (18/25). Hilum to left second bile duct confluence and tumor infiltration over left second bile duct confluence lengths in right-sided CIR were significantly shorter than those lengths in left-sided CIR (10.8 +/- 4.9 and 2.7 +/- 0.8 mm vs. 16.5 +/- 8.4 and 7.0 +/- 5.3 mm, respectively). Left-sided CIR patients had a marginally higher proportion of tumors invading < or =5 mm over the right second confluence than that in right-sided CIR patients (13/17 vs. 6/16; P = 0.061). The 3-year survival rate after CIR (28%) was significantly higher than after non-CIR (6.1%).
CONCLUSION
We recommend the criteria of CIR as bile duct variation type, length of hilum to contralateral second bile duct confluence, and extent of tumor infiltration over the second confluence for Bismuth type IV HCCA.
Keyword
Figure
-
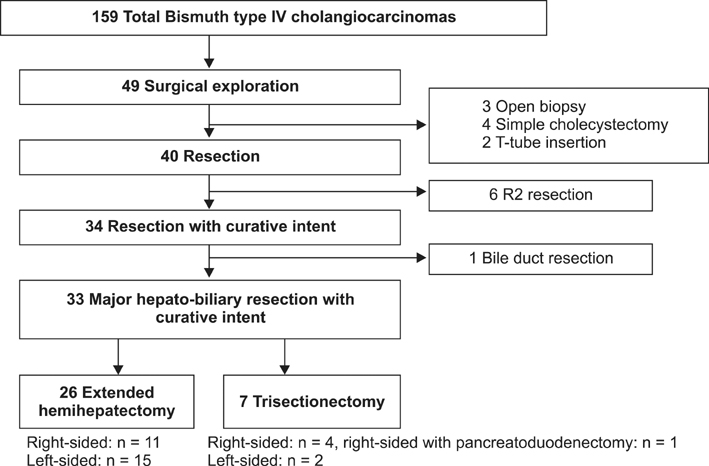
Fig. 1 Patients with Bismuth type IV hilar cholangiocarcinoma selected for curative-intended resection.
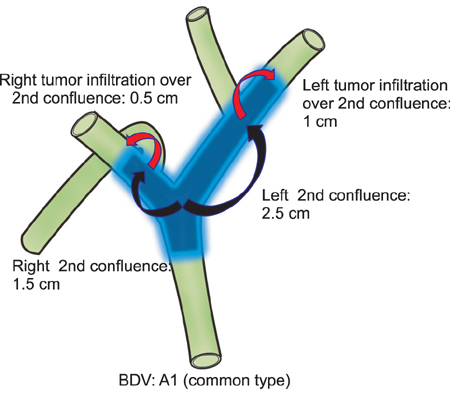
Fig. 2 Longitudinal measure of tumor extent in bile duct variation type A1. BDV, bile duct variation.
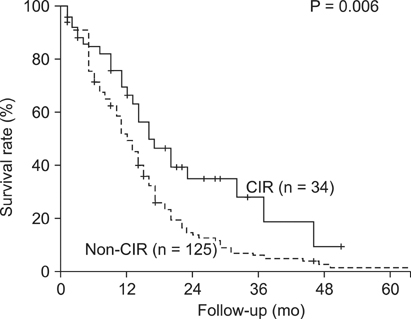
Fig. 3 Survival rate at follow-up in patients with Bismuth type IV hilar cholangiocarcinomas. CIR, major hepato-biliary resection with curative intent.
Cited by 2 articles
-
Comparison study for surgical outcomes of right versus left side hemihepatectomy to treat hilar cholangiocellular carcinoma
Seung Soo Hong, Dai Hoon Han, Gi Hong Choi, Jin Sub Choi
Ann Surg Treat Res. 2020;98(1):15-22. doi: 10.4174/astr.2020.98.1.15.Recent Updates in the Imaging Diagnosis of Cholangiocarcinoma
Ijin Joo
J Korean Soc Radiol. 2019;80(3):394-411. doi: 10.3348/jksr.2019.80.3.394.
Reference
-
1. Ito F, Cho CS, Rikkers LF, Weber SM. Hilar cholangiocarcinoma: current management. Ann Surg. 2009; 250:210–218.2. Neuhaus P, Jonas S, Bechstein WO, Lohmann R, Radke C, Kling N, et al. Extended resections for hilar cholangiocarcinoma. Ann Surg. 1999; 230:808–818.3. Hemming AW, Reed AI, Fujita S, Foley DP, Howard RJ. Surgical management of hilar cholangiocarcinoma. Ann Surg. 2005; 241:693–699.4. Ratti F, Cipriani F, Ferla F, Catena M, Paganelli M, Aldrighetti LA. Hilar cholangiocarcinoma: preoperative liver optimization with multidisciplinary approach. Toward a better outcome. World J Surg. 2013; 37:1388–1396.5. Bismuth H, Castaing D, Traynor O. Resection or palliation: priority of surgery in the treatment of hilar cancer. World J Surg. 1988; 12:39–47.6. Bismuth H, Corlette MB. Intrahepatic cholangioenteric anastomosis in carcinoma of the hilus of the liver. Surg Gynecol Obstet. 1975; 140:170–178.7. Aljiffry M, Abdulelah A, Walsh M, Peltekian K, Alwayn I, Molinari M. Evidence-based approach to cholangiocarcinoma: a systematic review of the current literature. J Am Coll Surg. 2009; 208:134–147.8. Sasaki R, Kondo T, Oda T, Murata S, Wakabayashi G, Ohkohchi N. Impact of three-dimensional analysis of multidetector row computed tomography cholangioportography in operative planning for hilar cholangiocarcinoma. Am J Surg. 2011; 202:441–448.9. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, editors. AJCC cancer staging manual. 7th ed. New York: Springer;2010.10. Seo H, Lee JM, Kim IH, Han JK, Kim SH, Jang JY, et al. Evaluation of the gross type and longitudinal extent of extrahepatic cholangiocarcinomas on contrast-enhanced multidetector row computed tomography. J Comput Assist Tomogr. 2009; 33:376–382.11. Ryoo I, Lee JM, Park HS, Han JK, Choi BI. Preoperative assessment of longitudinal extent of bile duct cancers using MDCT with multiplanar reconstruction and minimum intensity projections: comparison with MR cholangiography. Eur J Radiol. 2012; 81:2020–2026.12. Choi JY, Lee JM, Lee JY, Kim SH, Lee MW, Han JK, et al. Navigator-triggered isotropic three-dimensional magnetic resonance cholangiopancreatography in the diagnosis of malignant biliary obstructions: comparison with direct cholangiography. J Magn Reson Imaging. 2008; 27:94–101.13. Huang TL, Cheng YF, Chen CL, Chen TY, Lee TY. Variants of the bile ducts: clinical application in the potential donor of living-related hepatic transplantation. Transplant Proc. 1996; 28:1669–1670.14. Hiatt JR, Gabbay J, Busuttil RW. Surgical anatomy of the hepatic arteries in 1000 cases. Ann Surg. 1994; 220:50–52.15. Cheng YF, Huang TL, Lee TY, Chen TY, Chen CL. Variation of the intrahepatic portal vein; angiographic demonstration and application in living-related hepatic transplantation. Transplant Proc. 1996; 28:1667–1668.16. Kim MJ, Oh DY, Lee SH, Kim DW, Im SA, Kim TY, et al. Gemcitabine-based versus fluoropyrimidine-based chemotherapy with or without platinum in unresectable biliary tract cancer: a retrospective study. BMC Cancer. 2008; 8:374.17. Cheng Y, Chen Y, Chen H. Application of portal parenchyma-enterostomy after high hilar resection for Bismuth type IV hilar cholangiocarcinoma. Am Surg. 2010; 76:182–187.18. Endo I, Shimada H, Sugita M, Fujii Y, Morioka D, Takeda K, et al. Role of three-dimensional imaging in operative planning for hilar cholangiocarcinoma. Surgery. 2007; 142:666–675.19. Gwak HK, Kim WC, Kim HJ, Park JH. Extrahepatic bile duct cancers: surgery alone versus surgery plus postoperative radiation therapy. Int J Radiat Oncol Biol Phys. 2010; 78:194–198.20. Cheng Q, Luo X, Zhang B, Jiang X, Yi B, Wu M. Predictive factors for prognosis of hilar cholangiocarcinoma: postresection radiotherapy improves survival. Eur J Surg Oncol. 2007; 33:202–207.21. Jang JY, Kim SW, Park DJ, Ahn YJ, Yoon YS, Choi MG, et al. Actual long-term outcome of extrahepatic bile duct cancer after surgical resection. Ann Surg. 2005; 241:77–84.22. Kim S, Kim SW, Bang YJ, Heo DS, Ha SW. Role of postoperative radiotherapy in the management of extrahepatic bile duct cancer. Int J Radiat Oncol Biol Phys. 2002; 54:414–419.23. Liu CL, Fan ST, Lo CM, Tso WK, Lam CM, Wong J. Improved operative and survival outcomes of surgical treatment for hilar cholangiocarcinoma. Br J Surg. 2006; 93:1488–1494.24. Wakai T, Shirai Y, Moroda T, Yokoyama N, Hatakeyama K. Impact of ductal resection margin status on long-term survival in patients undergoing resection for extrahepatic cholangiocarcinoma. Cancer. 2005; 103:1210–1216.25. Paik KY, Choi DW, Chung JC, Kang KT, Kim SB. Improved survival following right trisectionectomy with caudate lobectomy without operative mortality: surgical treatment for hilar cholangiocarcinoma. J Gastrointest Surg. 2008; 12:1268–1274.26. Shimizu H, Kimura F, Yoshidome H, Ohtsuka M, Kato A, Yoshitomi H, et al. Aggressive surgical resection for hilar cholangiocarcinoma of the left-side predominance: radicality and safety of left-sided hepatectomy. Ann Surg. 2010; 251:281–286.27. Aloia TA, Charnsangavej C, Faria S, Ribero D, Abdalla EK, Vauthey JN, et al. High-resolution computed tomography accurately predicts resectability in hilar cholangiocarcinoma. Am J Surg. 2007; 193:702–706.28. Manfredi R, Barbaro B, Masselli G, Vecchioli A, Marano P. Magnetic resonance imaging of cholangiocarcinoma. Semin Liver Dis. 2004; 24:155–164.29. Chryssou E, Guthrie JA, Ward J, Robinson PJ. Hilar cholangiocarcinoma: MR correlation with surgical and histological findings. Clin Radiol. 2010; 65:781–788.30. Kim BS, Joo SH, Kim GY, Joo KR. Aggressive hilar inflammatory myofibroblastic tumor with hilar bile duct carcinoma in situ. J Korean Surg Soc. 2011; 81:Suppl 1. S59–S63.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- TNM Staging of Hilar Cholangiocarcinoma
- Comparison analysis of left-side versus right-side resection in bismuth type III hilar cholangiocarcinoma
- Surgical management of hilar cholangiocarcinoma: Controversies and recommendations
- Current Updates in the Surgical Management of Hilar Cholangiocarcinoma
- Analysis of Survival After Portal Vein Resection (PVR) In Combination With Hepatectomy For Hilar Cholangiocarcinoma: An Audit of 51 Cases
