Transcatheter Closures for Fistula Tract and Paravalvular Leak after Mitral Valve Replacement and Tricuspid Annuloplasty
- Affiliations
-
- 1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Division of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jksong@amc.seoul.kr
- 3Division of Cardiology, Daejeon St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea.
- KMID: 1859243
- DOI: http://doi.org/10.4070/kcj.2014.44.1.49
Abstract
- Paravalvular leaks (PVLs) often occur after surgical valve replacement. Surgical reoperation has been the gold standard of therapy for PVLs, but it carries a higher operative risk and an increased incidence of re-leaks compared to the initial surgery. In high surgical risk patients with appropriate geometries, transcatheter closure of PVLs could be an alternative to redo-surgery. Here, we report a case of successful staged transcatheter closures of a fistula tract between the aorta and right atrium, and mitral PVLs after mitral valve replacement and tricuspid annuloplasty.
Figure
-

Fig. 1 Transesophageal echocardiographic images showing shunt flow from the aorta to the right atrium. Shunt flow was evident on color Doppler flow mapping (A), and the diameter of the fistula (arrows) was 4 mm (B). Ao: aorta, LA: left atrium, RA: right atrium, RV: right ventricle.
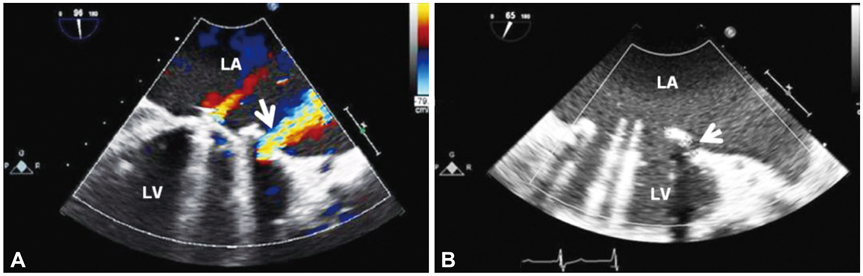
Fig. 2 Transesophageal echocardiographic images showing paravalvular leakage. Pathologic paravalvular mitral regurgitation jet (arrow) was evident at the lateral mitral annulus on color Doppler flow mapping (A), and the defect size was 4 mm (B). LA: left atrium, LV: left ventricle.
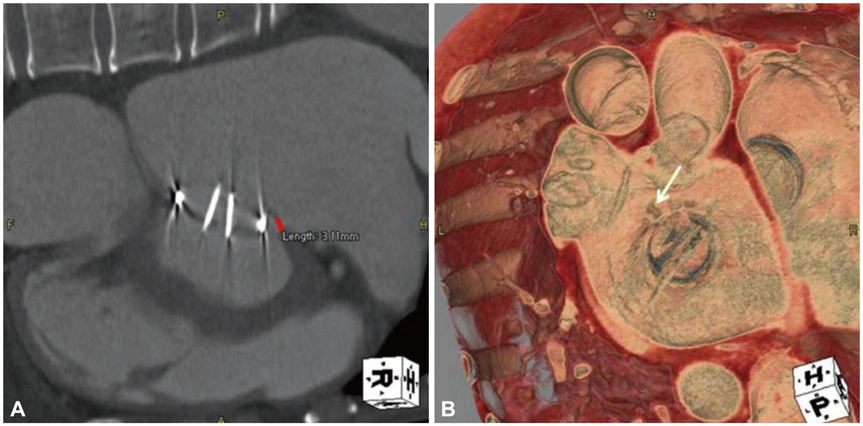
Fig. 3 Computed tomographic images showing paravalular leakage. The maximal defect size was 3 mm (A) and reconstructed images for the cardiac surgeons from the left atrial side showed that the defect was located at the antero-lateral mitral annulus (arrow, B).
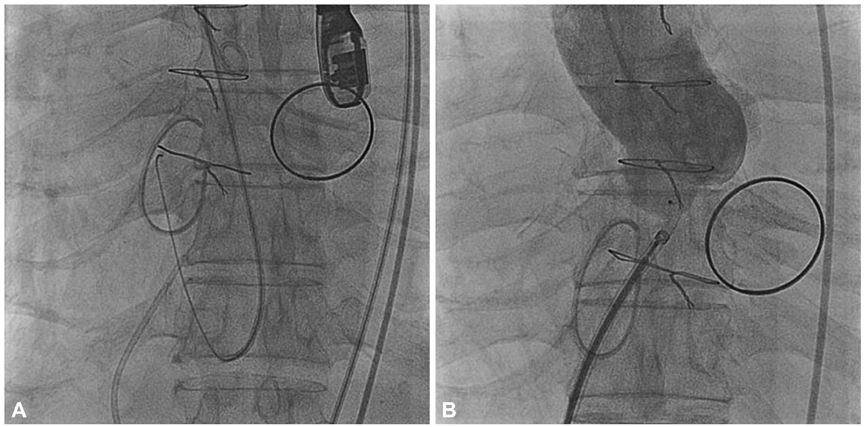
Fig. 4 Fluoroscopic images showing the procedure. A 6 Fr Cournand catheter was advanced into and passed through the defect from the aorta to the right atrium, and another 6 Fr Cournand catheter was introduced into the right atrium (A). An 8/6 mm sized Amplatzer duct occluder was deployed in the fistula tract from the aorta to the right atrium (B).
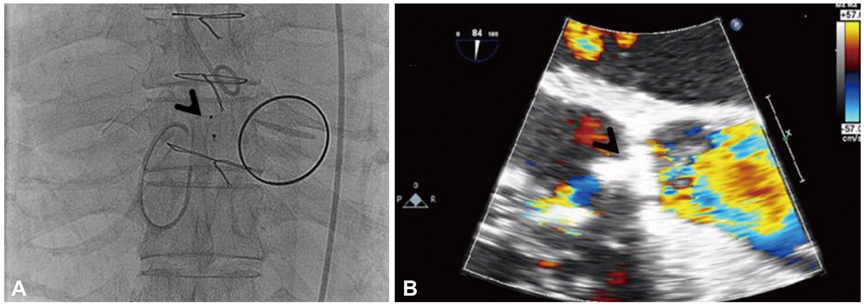
Fig. 5 Immediately after the procedure, both fluoroscopy (A) and transesophageal echocardiography (B) showed a well-positioned device and no remnant shunt (arrows).
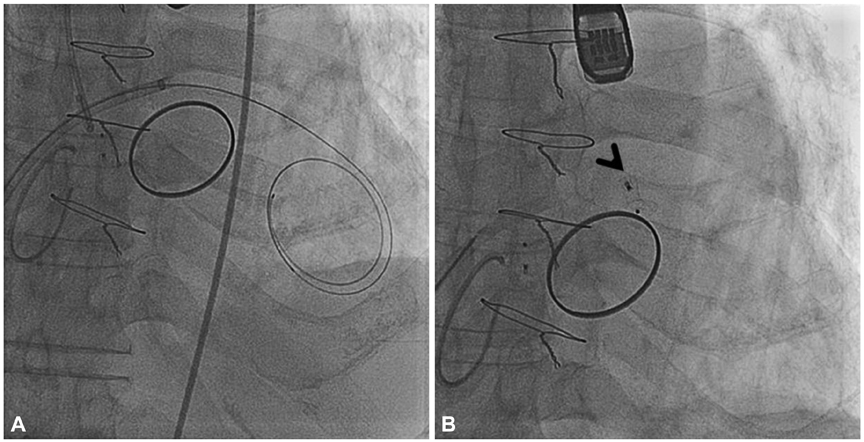
Fig. 6 Fluoroscopic images of the second procedure. After septal puncture (A), an 8/6 mm sized Amplatzer duct occluder was deployed in the tissue defect in the mitral annulus (arrow) (B).
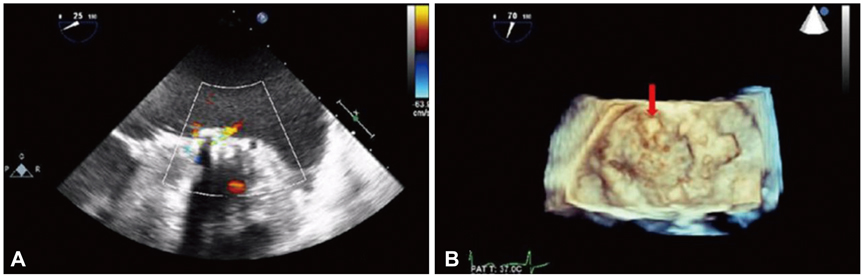
Fig. 7 Transesophageal echocardiographic images immediately after the procedure. Color Doppler flow mapping showed no remnant paravalvular leakage (A) and 3-dimensional echocardiography showed a well-positioned occluder (arrow) (B).
Reference
-
1. Kursaklioglu H, Barcin C, Iyisoy A, Baysan O, Celik T, Kose S. Percutaneous closure of mitral paravalvular leak via retrograde approach: with use of the Amplatzer duct occluder II and without a wire loop. Tex Heart Inst J. 2010; 37:461–464.2. Kuehl M, Schreieck J, Burgstahler C. Percutaneous closure of a periprosthetic leakage after mitral valve reoperation due to recurrent endocarditis. Catheter Cardiovasc Interv. 2009; 73:838–841.3. Pate GE, Al Zubaidi A, Chandavimol M, Thompson CR, Munt BI, Webb JG. Percutaneous closure of prosthetic paravalvular leaks: case series and review. Catheter Cardiovasc Interv. 2006; 68:528–533.4. Hourihan M, Perry SB, Mandell VS, et al. Transcatheter umbrella closure of valvular and paravalvular leaks. J Am Coll Cardiol. 1992; 20:1371–1377.5. Eisenhauer AC, Piemonte TC, Watson PS. Closure of prosthetic paravalvular mitral regurgitation with the Gianturco-Grifka vascular occlusion device. Catheter Cardiovasc Interv. 2001; 54:234–238.6. Webb JG, Pate GE, Munt BI. Percutaneous closure of an aortic prosthetic paravalvular leak with an Amplatzer duct occluder. Catheter Cardiovasc Interv. 2005; 65:69–72.7. Binder RK, Webb JG. Percutaneous mitral and aortic paravalvular leak repair: indications, current application, and future directions. Curr Cardiol Rep. 2013; 15:342.8. Nietlispach F, Johnson M, Moss RR, et al. Transcatheter closure of paravalvular defects using a purpose-specific occluder. JACC Cardiovasc Interv. 2010; 3:759–765.9. Pate GE, Thompson CR, Munt BI, Webb JG. Techniques for percutaneous closure of prosthetic paravalvular leaks. Catheter Cardiovasc Interv. 2006; 67:158–166.10. Cortés M, García E, García-Fernandez MA, Gomez JJ, Perez-David E, Fernández-Avilés F. Usefulness of transesophageal echocardiography in percutaneous transcatheter repairs of paravalvular mitral regurgitation. Am J Cardiol. 2008; 101:382–386.11. Kort HW, Sharkey AM, Balzer DT. Novel use of the Amplatzer duct occluder to close perivalvar leak involving a prosthetic mitral valve. Catheter Cardiovasc Interv. 2004; 61:548–551.12. Shapira Y, Hirsch R, Kornowski R, et al. Percutaneous closure of perivalvular leaks with Amplatzer occluders: feasibility, safety, and shortterm results. J Heart Valve Dis. 2007; 16:305–313.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Trido Mitral Valve Replacement with Dacron Collar Prosthetic Valve due to Paravalvular Leak
- ITBI Repair of Paravalvular Leak at Mitral Position after Redo DVR
- Left Atrial Wall Dissection after Mitral Valve Replacement
- Hemodynamic Improvement after Surgical Intervention for Pannus in Prosthetic Mitral Valve
- Comparable Outcomes of Bicuspid Aortic Valves for RapidDeployment Aortic Valve Replacement
