An asymptomatic ovarian steroid cell tumor with complete cystic morphology: A case report
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Seoul Medical Center, Seoul, Korea. harmony4@catholic.ac.kr
- KMID: 1857187
- DOI: http://doi.org/10.5468/OGS.2013.56.1.50
Abstract
- Steroid cell tumors of the ovary are extremely rare, accounting for only 0.1% of all ovarian tumors. Of these, steroid cell tumors, not otherwise specified (NOS) constitute about 56% of all steroid cell tumors. Most steroid cell tumors secrete steroid hormones, and only about 10% to 15% of patients are asymptomatic. The morphology of steroid cell tumors, NOS is predominantly reported to be solid, and a review of case reports from 1979 until now revealed only 5 cases that were mainly cystic tumors. The present case, in a patient who had undergone a previous hysterectomy and surgery for a peritoneal inclusion cyst, is reported due to its rarity and its unusual presentation, together with a brief review of the literature. The tumor showed no clinical signs and symptoms typical of a steroid hormone secreting tumor and had an atypical morphology, being primarily multi-septate cystic with a minor solid portion.
Keyword
MeSH Terms
Figure
-

Fig. 1 Transvaginal ultrasound indicating a large 10×8×7 cm3 sized cystic mass at the center of the pelvic cavity, with internal septation and no apparent solid portion.
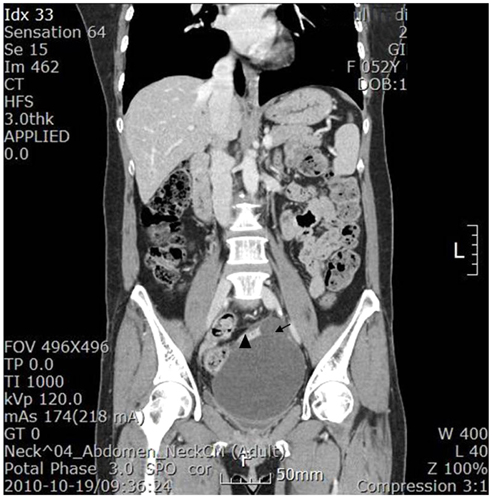
Fig. 2 An abdominopelvic computed tomographic scan after enhancement shows a 10×8 cm sized cystic mass in the left ovary, with internal septation (arrow) and a solid portion (arrowhead), which is enhanced by contrast media.
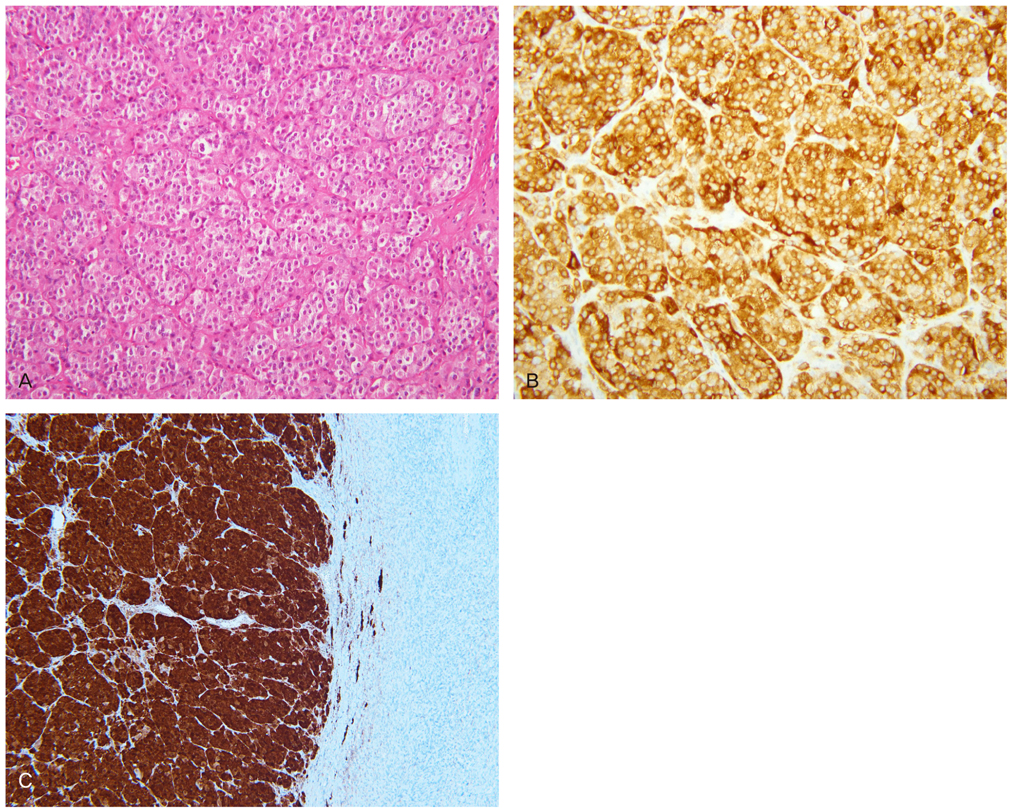
Fig. 3 (A) Histological specimen shows large aggregates of tumor cells with abundant eosinophilic to clear cytoplasm, with a granular appearance and vacuolization (H&E, ×200). (B) Immunohistochemical staining shows the tumor cells exhibiting a diffuse positive reaction for inhibin (brown) (×200). (C) Immunohistochemical staining shows a diffuse positive reaction of the tumor cells for calretinin (dark red) (×100).
Reference
-
1. Young RH. Kurman RJ, Ellenson LH, Ronnett BM, editors. Sex cord-stromal, steroid cell, and other ovarian tumors with endocrine, paraendocrine, and paraneoplastic manifestations. Blaustein's pathology of the female genital tract. 2011. 6th ed. Boston (MA): Springer;785–846.2. Hayes MC, Scully RE. Ovarian steroid cell tumors (not otherwise specified). A clinicopathological analysis of 63 cases. Am J Surg Pathol. 1987. 11:835–845.3. Gershenson DM, Hartmann LC, Young RH. Barakat RR, editor. Ovarian sex cord-stromal tumors. Principles and practice of gynecologic oncology. 2009. 5th ed. Philadelphia (PA): Lippencott;855–874.4. Baloglu A, Bezircioglu I, Cetinkaya B, Karci L, Bicer M. Development of secondary ovarian lesions after hysterectomy without oophorectomy versus unilateral oophorectomy for benign conditions: a retrospective analysis of patients during a nine-year period of observation. Clin Exp Obstet Gynecol. 2010. 37:299–302.5. Taylor HB, Norris HJ. Lipid cell tumors of the ovary. Cancer. 1967. 20:1953–1962.6. Deavers MT, Malpica A, Ordonez NG, Silva EG. Ovarian steroid cell tumors: an immunohistochemical study including a comparison of calretinin with inhibin. Int J Gynecol Pathol. 2003. 22:162–167.7. Young RH, Shully RE. Haines M, Taylor CW, Fox H, Wells M, editors. Steroid cell tumors of the ovary. Haines and Tayler obstetrical and gynaecological pathology. 2003. 5th ed. Edinburgh: Churchill Livingstone;845–856.8. Wang PH, Chao HT, Lee RC, Lai CR, Lee WL, Kwok CF, et al. Steroid cell tumors of the ovary: clinical, ultrasonic, and MRI diagnosis: a case report. Eur J Radiol. 1998. 26:269–273.9. Wang PH, Chao HT, Liu RS, Cho YH, Ng HT, Yuan CC. Diagnosis and localization of testosterone-producing ovarian tumors: imaging or biochemical evaluation. Gynecol Oncol. 2001. 83:596–598.10. Sakamoto K, Fujimitsu R, Ida M, Horiuchi S, Hamada Y, Yoshimitsu K. MR diagnosis of steroid cell tumor of the ovary: value of chemical shift imaging. Magn Reson Med Sci. 2009. 8:193–195.11. Wang PH, Chao HT, Lee WL. Use of a long-acting gonadotropin-releasing hormone agonist for treatment of steroid cell tumors of the ovary. Fertil Steril. 1998. 69:353–355.12. Bernasconi D, Del Monte P, Marinaro E, Marugo A, Marugo M. Severe postmenopausal hyperandrogenism due to an ovarian lipoid cell tumor: a case report. Minerva Endocrinol. 2004. 29:25–29.13. Cserepes E, Szucs N, Patkos P, Csapo Z, Molnar F, Toth M, et al. Ovarian steroid cell tumor and a contralateral ovarian thecoma in a postmenopausal woman with severe hyperandrogenism. Gynecol Endocrinol. 2002. 16:213–216.14. Kim YT, Kim SW, Yoon BS, Kim SH, Kim JH, Kim JW, et al. An ovarian steroid cell tumor causing virilization and massive ascites. Yonsei Med J. 2007. 48:142–146.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hematometra Due to Cervical Stenosis in a Postmenopausal Woman with Incidental Ovarian Steroid Cell Tumor: A Case Report
- Laparoscopic management of asymptomatic ovarian steroid cell tumors, not otherwise specified: A case report and literature review
- Recurrent ovarian steroid cell tumor, not otherwise specified managed with debulking surgery, radiofrequency ablation, and adjuvant chemotherapy
- A Case of Ovarian Steroid Cell Tumor, Not Otherwise Specified, Treated with Surgery and Gonadotropin Releasing Hormone Agonist
- Ovarian serous cystadenoma associated with Sertoli-Leydig cell tumor: a case report
