J Korean Diabetes.
2011 Mar;12(1):2-5. 10.4093/jkd.2011.12.1.2.
Outcome Research in Diabetes
- Affiliations
-
- 1Department of Endocrinology and Metabolism, Ajou University, School of Medicine, Suwon, Korea. LKW65@ajou.ac.kr
- KMID: 1851894
- DOI: http://doi.org/10.4093/jkd.2011.12.1.2
Abstract
- Economic development has lead to increased life expectancy, population growth, and spread of the Western life style, resulting in a gradual increase of diabetic patients during the last three decades. Outcome research focusing on the economics of the medical field began in mid the 1990s, including publications about costs, cost-effectiveness analysis, and policy reflection. According to the ADA, direct cost spending on diabetes was $91.8 billion in 2002 and is projected to be $156 billion in 2010 and $192 billion in 2020. In Canada, research found that the direct cost of diabetic care was $2.6 million (American dollars) in 1998, 7.8% of the total Canadian medical expenditure. Half of this cost was incurred in hospitals (IPD: 19%, medication: 31%). Recent domestic studies have analyzed the expenses associated with type 2 diabetes in some general hospitals. Type 2 diabetic patients, without complication, spend about 1,184,563 won annually on healthcare. On the other hand, patients with microvascular diseases spend up to 4.7 times as much, and patients with macrovascular disease incur up to 10.7 times greater costs. Patients with both complications have been shown to pay 8.8 times more than do those with no complications. The increased costs charged to kidney transplant patients was about 23.1 times greater than for those with no complications, while dialysis increased costs by 21 times, macrovascular disease with PTCA or CABG resulted in a 12.4-fold increase, and BKA was 11.8-fold more expensive. The total medical costs have soared with the treatment progress of diabetic retinopathy or nephropathy. In diabetic treatments, complication occurrence ultimately has an effect on the QOL, the patient mortality, and is associated with the direct medical expenses. Thus it is critical not to delay care in diabetic patients in order to avoid increased direct medical costs. Therefore, in diabetic care, as outlined in the medical care plan policy, it is most critical to adequately control blood sugar, blood pressure, and cholesterol in conjunction with the early discovery of any complications through the appropriate management techniques.
Keyword
MeSH Terms
Figure
-
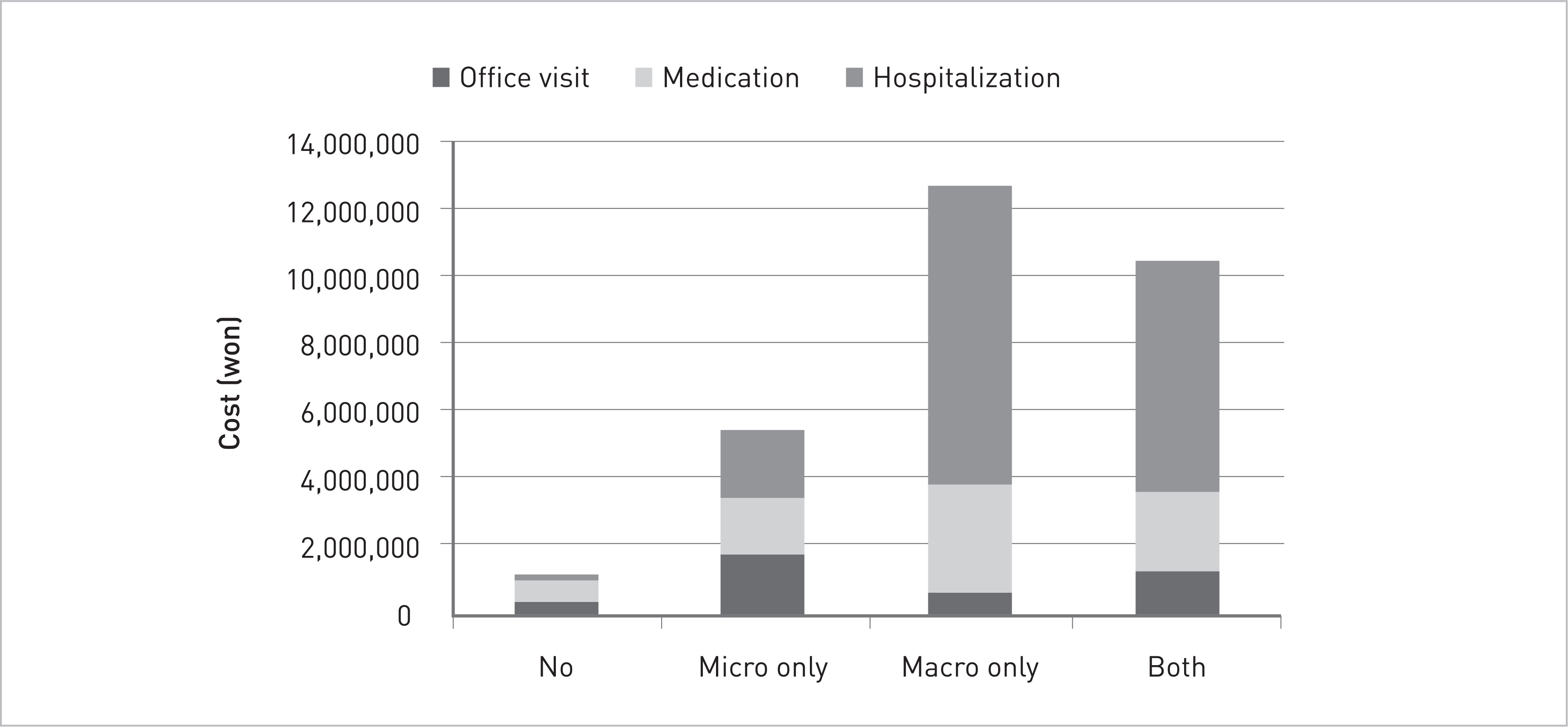
Fig. 1. Annual medical costs per patient according to the presence of diabetic complications.
Cited by 1 articles
-
The Epidemiology of Diabetic Nephropathy
Jin Hwa Kim
J Korean Diabetes. 2013;14(1):11-14. doi: 10.4093/jkd.2013.14.1.11.
Reference
-
1. Sicree R, Shaw J, Zimmet P. Diabetes atlas. 2nd ed.Brussels: International Diabetes Federation;2003. p. 15–71.2. Kim KS, Choi CH, Lee DY, Kim EJ. Epidemiological study on diabetes mellitus among rural Korean. Korean Diabetes J. 1972; 1:17–24.3. Korea Centers for Disease Control and Prevention. The Third Korea National Health and Nutrition Examination Survey (KNHANES III), 2005: Illness of Adults. Seoul: Korea Centers for Disease Control and Prevention;2006.4. Annemans L. Pharmacoeconomics for decision-markers. In: ISPOR 10th Annual European Congress;. 2007. Oct 20-23; Dublin, IE.5. Zhang P, Engelgau MM, Norris SL, Gregg EW, Narayan KM. Application of economic analysis to diabetes and diabetes care. Ann Intern Med. 2004; 140:972–7.
Article6. Hogan P, Dall T, Nikolov P. Economic costs of diabetes in the US in 2002. Diabetes Care. 2003; 26:917–32.7. Dawson KG, Gomes D, Gerstein H, Blanchard JF, Kahler KH. The economic cost of diabetes in Canada, 1998. Diabetes Care. 2002; 25:1303–7.
Article8. Williams R, Van Gaal L, Lucioni C. Assessing the impact of complications on the costs of Type II diabetes. Diabetologia. 2002; 45:S13–7.
Article9. Brandle M, Zhou H, Smith BR, Marriott D, Burke R, Tabaei BP, Brown MB, Herman WH. The direct medical cost of type 2 diabetes. Diabetes Care. 2003; 26:2300–4.
Article10. Clarke P, Gray A, Legood R, Briggs A, Holman R. The impact of diabetes-related complications on healthcare costs: results from the United Kingdom Prospective Diabetes Study (UKPDS Study No. 65). Diabet Med. 2003; 20:442–50.
Article11. O'Brien JA, Patrick AR, Caro JJ. Cost of managing complications resulting from type 2 diabetes mellitus in Canada. BMC Health Serv Res. 2003; 3:7.12. Caro JJ, Ward AJ, O'Brien JA. Lifetime costs of complications resulting from type 2 diabetes in the U.S. Diabetes Care. 2002; 25:476–81.
Article13. American Diabetes Association. Standards of medical care in diabetes-2006. Diabetes Care. 2006; 29(Suppl 1):S4–42.14. Moon EJ, Jo YE, Park TC, Kim YK, Jung SH, Kim HJ, Kim DJ, Chung YS, Lee KW. Clinical characteristics and direct medical costs of type 2 diabetic patients. Korean Diabetes J. 2008; 32:358–65.
Article15. Hwang JA, Park TC, Jung SH, Kim HJ, Kim DJ, Kim SH, Nam MS, Kim TH, Lee MK, Lee KW. Direct medical costs of type 2 diabetic patients in the tertiary hospital. Korean Diabetes J. 2008; 32:259–68.
Article16. Chun KH, Lee KW, Kim DJ, Kim HJ, Paek KW, Lee SJ. An analysis of medical costs of diabetic patients in a university hospital (1996~2005). Korean Diabetes J. 2008; 32:366–76.
Article
