Multidrug-Resistant Tuberculosis Presenting as Miliary Tuberculosis without Immune Suppression: A Case Diagnosed Rapidly with the Genotypic Line Probe Assay Method
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. ymleeim@paik.ac.kr
- 2Department of Pulmonology, Samsung Changwon Medical Center, Sungkyunkwan University School of Medicine, Changwon, Korea.
- 3Department of Laboratory Medicine, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 4Department of Radiology, Inje University Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 1842972
- DOI: http://doi.org/10.4046/trd.2014.76.5.245
Abstract
- Miliary tuberculosis (TB) is a rare extrapulmonary form of TB, and there have been only two reports of miliary TB associated with infection with multidrug-resistant (MDR)-TB pathogen in an immunocompetent host. A 32-year-old woman was referred to our hospital because of abnormal findings on chest X-ray. The patient was diagnosed with MDR-TB by a line probe assay and was administered proper antituberculous drugs. After eight weeks, a solid-media drug sensitivity test revealed that the pathogen was resistant to ethambutol and streptomycin in addition to isoniazid and rifampicin. The patient was then treated with effective antituberculous drugs without delay after diagnosis of MDR-TB. To the best of our knowledge, this is the first case of miliary TB caused by MDR-TB pathogen in Korea.
MeSH Terms
Figure
-
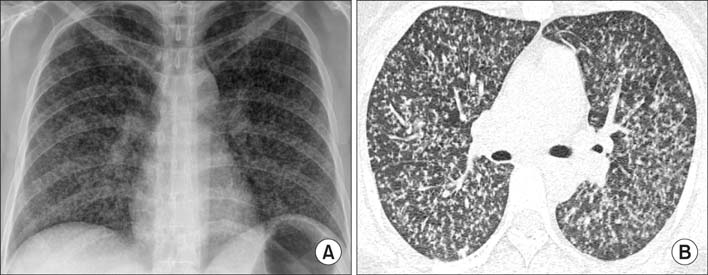
Figure 1 A 32-year-old woman diagnosed as military tuberculosis caused by multidrug-resistant pathogen. (A) Chest radiograph at the time of presentation showed diffuse micro-nodules involving both lung fields. (B) High-resolution computed tomography image (1.0 mm section thickness) revealed uniform-sized small nodules randomly distributed throughout both lungs.
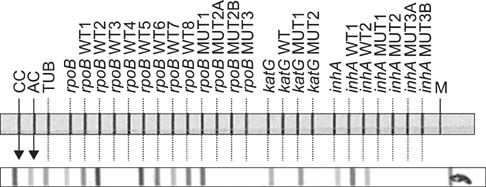
Figure 2 Line probe assay results: for rifampicin, the strain revealed negative results of rpoB WT3 and WT4 probes, and positive result of rpoB MUT1 probe for D516V mutation; for isoniazid, there were missing band of katG WT and additional positive band in katG MUT1 for S315T1 mutation.

Figure 3 A chest radiography after treatment showed resolution of diffuse micro-nodules involving both lung fields.
Reference
-
1. Gandhi NR, Nunn P, Dheda K, Schaaf HS, Zignol M, van Soolingen D, et al. Multidrug-resistant and extensively drug-resistant tuberculosis: a threat to global control of tuberculosis. Lancet. 2010; 375:1830–1843.2. Falzon D, Jaramillo E, Schunemann HJ, Arentz M, Bauer M, Bayona J, et al. WHO guidelines for the programmatic management of drug-resistant tuberculosis: 2011 update. Eur Respir J. 2011; 38:516–528.3. World Health Organization. WHO/HTM/TB/2006.361. Guidelines for the programmatic management of drug-resistant tuberculosis. Geneva: WHO;2006.4. Centers for Disease Control and Prevention. Reported tuberculosis in the United States, 2010. Atlanta: Centers for Disease Control and Prevention;2011.5. Daikos GL, Uttamchandani RB, Tuda C, Fischl MA, Miller N, Cleary T, et al. Disseminated miliary tuberculosis of the skin in patients with AIDS: report of four cases. Clin Infect Dis. 1998; 27:205–208.6. Hill AR, Premkumar S, Brustein S, Vaidya K, Powell S, Li PW, et al. Disseminated tuberculosis in the acquired immunodeficiency syndrome era. Am Rev Respir Dis. 1991; 144:1164–1170.7. Shah A, Panjabi C, Maurya V, Khanna P. Multidrug resistant miliary tuberculosis and Pott's disease in an immunocompetent patient. Saudi Med J. 2004; 25:1468–1470.8. Sasse J, Teichmann D. Disseminated multiorgan MDR-TB resistant to virtually all first-line drugs. Eur Respir Rev. 2009; 18:291–294.9. Kim SY, Kim HJ, Kim CK, Yoon HR, Bae HG, Lee SH, et al. The recent status of multidrug- and extensively drug-resistant tuberculosis in Korea. Tuberc Respir Dis. 2010; 68:146–154.10. Caminero JA. Multidrug-resistant tuberculosis: epidemiology, risk factors and case finding. Int J Tuberc Lung Dis. 2010; 14:382–390.11. Kim JH, Langston AA, Gallis HA. Miliary tuberculosis: epidemiology, clinical manifestations, diagnosis, and outcome. Rev Infect Dis. 1990; 12:583–590.12. Ray S, Talukdar A, Kundu S, Khanra D, Sonthalia N. Diagnosis and management of miliary tuberculosis: current state and future perspectives. Ther Clin Risk Manag. 2013; 9:9–26.13. Ahmad S, Mokaddas E. Recent advances in the diagnosis and treatment of multidrug-resistant tuberculosis. Respir Med. 2009; 103:1777–1790.14. Morgan M, Kalantri S, Flores L, Pai M. A commercial line probe assay for the rapid detection of rifampicin resistance in Mycobacterium tuberculosis: a systematic review and meta-analysis. BMC Infect Dis. 2005; 5:62.15. Bwanga F, Hoffner S, Haile M, Joloba ML. Direct susceptibility testing for multi drug resistant tuberculosis: a meta-analysis. BMC Infect Dis. 2009; 9:67.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Direct Detection of Rifampin-Resistant Mycobacterium Tuberculosis by Polymerase Chain Reaction and Line Probe Assay in Sputums
- Differentiating between Intestinal Tuberculosis and Crohn’s Disease May Be Complicated by Multidrug-resistant Mycobacterium tuberculosis
- Early Detection of Mycobacterium Tuberculosis and Determination Rifampin-Resistance by PCR-Reverse Hybridization (Line Probe Assay) v
- Immune Reconstitution Inflammatory Syndrome Presenting as Cutaneous Miliary Tuberculosis in an HIV-Infected Patient
- Multidrug-resistant Tuberculosis Spondylitis: A Case Report
