Korean J Obstet Gynecol.
2012 Jan;55(1):55-58. 10.5468/KJOG.2012.55.1.55.
Isolated torsion of bilateral fallopian tubes combined with tubal endometriosis: A case report
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Keimyung University School of Medicine, Daegu, Korea. r1670416@dsmc.or.kr
- KMID: 1836766
- DOI: http://doi.org/10.5468/KJOG.2012.55.1.55
Abstract
- Torsion of the fallopian tube is less frequent. Indeed, isolated bilateral fallopian tube torsion is rare and often difficult to diagnose. The etiology of fallopian tube torsion is still uncertain, especially when this is not associated with torsion of the ovary. We present a case of the torsion of isolated bilateral fallopian tube combined with tubal endometriosis. A 30-year-old woman presented with chronic abdominal pain of 5-month duration and severe dysmenorrhea. Presumptive diagnosis by ultrasound and magnetic resonance imaging was both adnexal endometriosis. At laparoscopy, the fimbrial ends of both tubes were dilated, twisted and necrotic changes with adhesion to omentum, which subsequently led to terminal obstruction of that tube. However, both ovaries and uterus were normal. Laparoscopic bilateral salpingectomy was performed. The postoperative histological report confirmed hematosalpinx with tubal endometriosis. To our knowledge, this is the first case of isolated and bilateral fallopian tubes torsion combined with tubal endometriosis.
Keyword
MeSH Terms
Figure
-
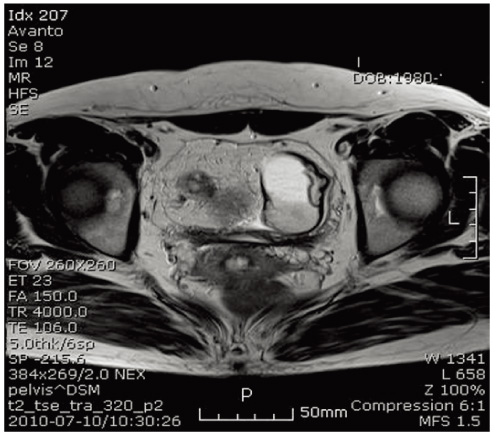
Fig. 1 Pelvic magnetic resonance imaging (MRI). Axial MRI view of the pelvis.
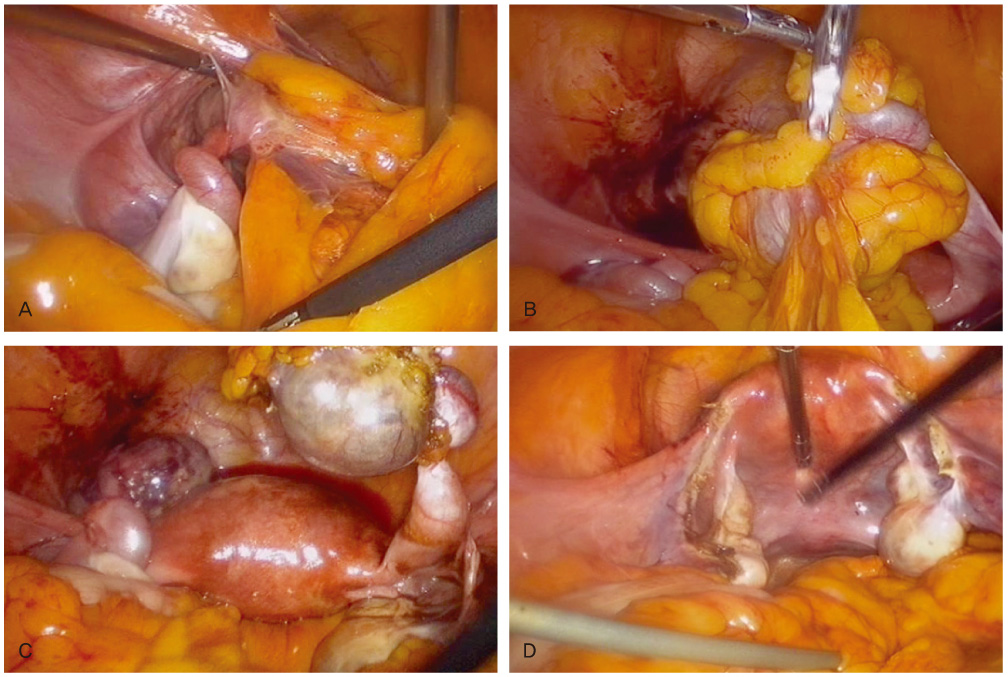
Fig. 2 Laparoscopic views. (A) The lesion of torsion of the left fallopian tube. The fimbrial end of the left tube was adherent to the omentum and pelvic wall. (B) Adhesion of the torted right fallopian tube with the omentum. (C) Laparoscopic pelvic overview after adhesiolysis shows bilateral torted tubes and cystic dilatation at the distal portion. (D) Laparoscopic pelvic overview after bilateral salpingectomy shows normal uterus and both ovaries.
Reference
-
1. Rizk DE, Lakshminarasimha B, Joshi S. Torsion of the fallopian tube in an adolescent female: a case report. J Pediatr Adolesc Gynecol. 2002. 15:159–161.2. Comerci G, Colombo FM, Stefanetti M, Grazia G. Isolated fallopian tube torsion: a rare but important event for women of reproductive age. Fertil Steril. 2008. 90:1198.e23–1198.e25.3. Wong SW, Suen SH, Lao T, Chung KH. Isolated fallopian tube torsion: a series of six cases. Acta Obstet Gynecol Scand. 2010. 89:1354–1356.4. Ohara N, Narita F, Murao S. Isolated torsion of haematosalpinx associated with tubal endometriosis. J Obstet Gynaecol. 2003. 23:453–454.5. Youssef AF, Fayad MM, Shafeek MA. Torsion of the fallopian tube. A clinico-pathological study. Acta Obstet Gynecol Scand. 1962. 41:292–309.6. Phillips K, Fino ME, Kump L, Berkeley A. Chronic isolated fallopian tube torsion. Fertil Steril. 2009. 92:394.e1–394.e3.7. van der Zanden M, Nap A, van Kints M. Isolated torsion of the fallopian tube: a case report and review of the literature. Eur J Pediatr. 2011. 170:1329–1332.8. Lo LM, Chang SD, Lee CL, Liang CC. Clinical manifestations in women with isolated fallopian tubal torsion; a rare but important entity. Aust N Z J Obstet Gynaecol. 2011. 51:244–247.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Torsion of Fallopian Tubes: Detection of Pedicle at Tubal End: Two Case Report
- Isolated Fallopian Tubal To rsion: A Case Report
- Isolated tubal torsion with diagnosed hydrosalpinx
- Isolated torsion of the hydrosalpinx after hysterectomy: A case report
- Microscopic lesions of fallopian tubes in endometrioid carcinoma of the endometrium: How effective are the macroscopic tubal sampling techniques?
