Unusual Left Ventricular Endocardial Metastasis from Primary Lung Cancer
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Seoul, Korea. grhong@yuhs.ac
- KMID: 1808353
- DOI: http://doi.org/10.4250/jcu.2012.20.3.157
Abstract
- The heart is frequently the site of metastasis of various malignant tumors. Lung cancer is one of the most common primary tumors of cardiac metastasis and usually involves the pericardium or epicardium by direct invasion and/or lymphatic spread. However, metastasis of lung cancer involving the left ventricular endocardium is extremely rare. We report a patient with adenocarcinoma of lung, metastasized to the left ventricular myocardium and endocardium, diagnosed by echocardiography and 18-fludeoxyglucose positron emission tomography-computed tomography.
Keyword
MeSH Terms
Figure
-
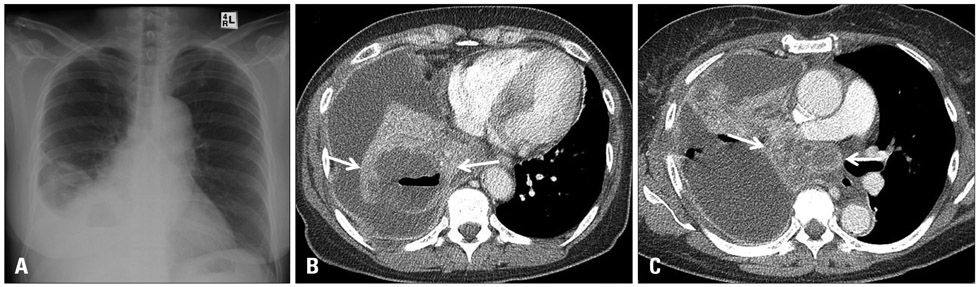
Fig. 1 Chest X-ray and computed tomography findings of lung lesion. Soft tissue fullness at right infra-hilar area and air-fluid level in right lower lung field (A). Cavitary lung mass with inner low density and multilocular effusion in the right lower lobe (B: white arrows) and multiple lymphadenopathies in right side mediastinum (C: white arrows).

Fig. 2 Transthoracic echocardiography findings of left ventricular mass in parasternal long axis (A) and apical 4 chamber view (B). Hyper-mobile, 2.4 cm × 1.4 cm sized mass is attached at interventricular septum of left ventricular outflow tract (white arrows). Apical long axis view (C) and zoom image (D) of left ventricular mass. Multi-lobulated, cystic nature mass with stalk (D: white arrow) is well visualized.
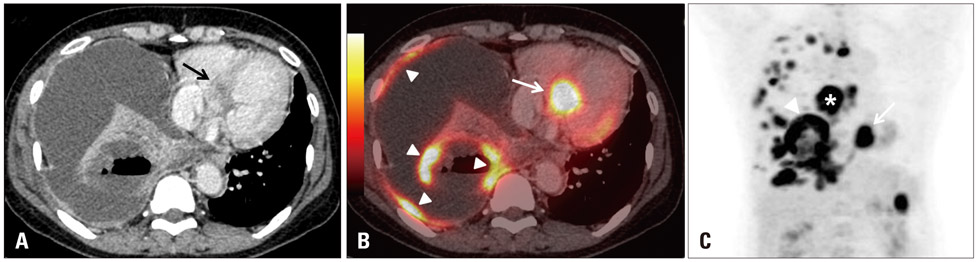
Fig. 3 18-fludeoxyglucose (FDG) positron emission tomography-computed tomography image of left ventricular mass and lung mass. The low density lesion in interventricular septum (A: black arrow) showed intense FDG uptake [B: white arrow, maximal standardized uptake value (SUVmax) = 13.9]. Primary lung cancer (SUVmax = 14.8) and multiple pleural metastasis also showed intense FDG uptake (B: white arrowheads). Coronal section image (C) showing multiple FDG uptake in primary lung cancer (white arrowhead), mediastinal lymph node (*), and the heart (white arrow).
Reference
-
1. Reynen K, Köckeritz U, Strasser RH. Metastases to the heart. Ann Oncol. 2004. 15:375–381.
Article2. Klatt EC, Heitz DR. Cardiac metastases. Cancer. 1990. 65:1456–1459.
Article3. Abe S, Watanabe N, Ogura S, Kunikane H, Isobe H, Yamaguchi E, Munakata M, Kawakami Y. Myocardial metastasis from primary lung cancer: myocardial infarction-like ECG changes and pathologic findings. Jpn J Med. 1991. 30:213–218.
Article4. Bussani R, De-Giorgio F, Abbate A, Silvestri F. Cardiac metastases. J Clin Pathol. 2007. 60:27–34.
Article5. Che GW, Liu LX, Zhang EY, Zhou QH. Left ventricular metastasis from a primary lung carcinoma. Chin Med J (Engl). 2007. 120:2323–2324.
Article6. Strauss BL, Matthews MJ, Cohen MH, Simon R, Tejada F. Cardiac metastases in lung cancer. Chest. 1977. 71:607–611.
Article7. Bisel HF, Wroblewski F, Ladue JS. Incidence and clinical manifestations of cardiac metastases. J Am Med Assoc. 1953. 153:712–715.
Article8. Tamura A, Matsubara O, Yoshimura N, Kasuga T, Akagawa S, Aoki N. Cardiac metastasis of lung cancer. A study of metastatic pathways and clinical manifestations. Cancer. 1992. 70:437–442.
Article9. Kasai T, Kishi K, Kawabata M, Narui K, Momomura S, Yoshimura K. Cardiac metastasis from lung adenocarcinoma causing atrioventricular block and left ventricular outflow tract obstruction. Chest. 2007. 131:1569–1572.
Article10. Deetjen A, Conradi G, Möllmann S, Kluge A, Hamm CW, Dill T. Cardiac metastasis of a renal cell adenocarcinoma investigated by cardiac magnetic resonance imaging. Clin Res Cardiol. 2006. 95:492–495.
Article11. Vind SH, Hess S. Possible role of PET/CT in infective endocarditis. J Nucl Cardiol. 2010. 17:516–519.
Article12. Bryant AS, Cerfolio RJ. The maximum standardized uptake values on integrated FDG-PET/CT is useful in differentiating benign from malignant pulmonary nodules. Ann Thorac Surg. 2006. 82:1016–1020.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Primary Leiomyosarcoma of the Left Lower Posterior Chest wall with Lung Metastasis: One Case Report
- Lung Cancer Recurrence with Solitary Pancreatic Metastasis Mimicking Primary Pancreatic Cancer
- Two Cases of Uveal Metastasis of Lung Cancer with Systemic Metastasis
- Gastric Metastasis of Primary Lung Adenocarcinoma Mistaken for Primary Gastric Cancer
- Abnormal morphological patterns of the left ventricular myocardium in the critical stenosis of the aortic valve and the intact ventricular septum
