Partial Visual Rehabilitation Using a Toric Implantable Collamer Lens in a Patient with Keratoconus: A Case Report with 20 Months of Follow-up
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea. kmk9@snu.ac.kr
- 2Laboratory of Corneal Regenerative Medicine and Immunology, Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul, Korea.
- 3Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 1798061
- DOI: http://doi.org/10.3341/kjo.2013.27.3.211
Abstract
- We report the case of a 37-year-old man with a high myopic keratoconus eye that was treated with a posterior chamber toric implantable collamer lens (ICL) in Korea. The patient had a history of contact lens intolerance and did not want to have a corneal transplantation. His uncorrected visual acuity (UCVA) and best spectacle corrected visual acuity were 0.02 and 0.4 in the left eye, respectively. Preoperatively, the manifest refraction was -12.0 -3.5 x 30A. Postoperatively, the manifest refraction was -1.75 x 180A. UCVA improved markedly after implantation. No intraoperative or postoperative complications were observed during 20 months of follow-up. Toric ICL implantation may be a possible alternative surgical option for the visual rehabilitation of high myopic astigmatism in keratoconus patients with rigid gas permeable contact lens intolerance and in patients who do not want to get a corneal transplant.
MeSH Terms
Figure
-
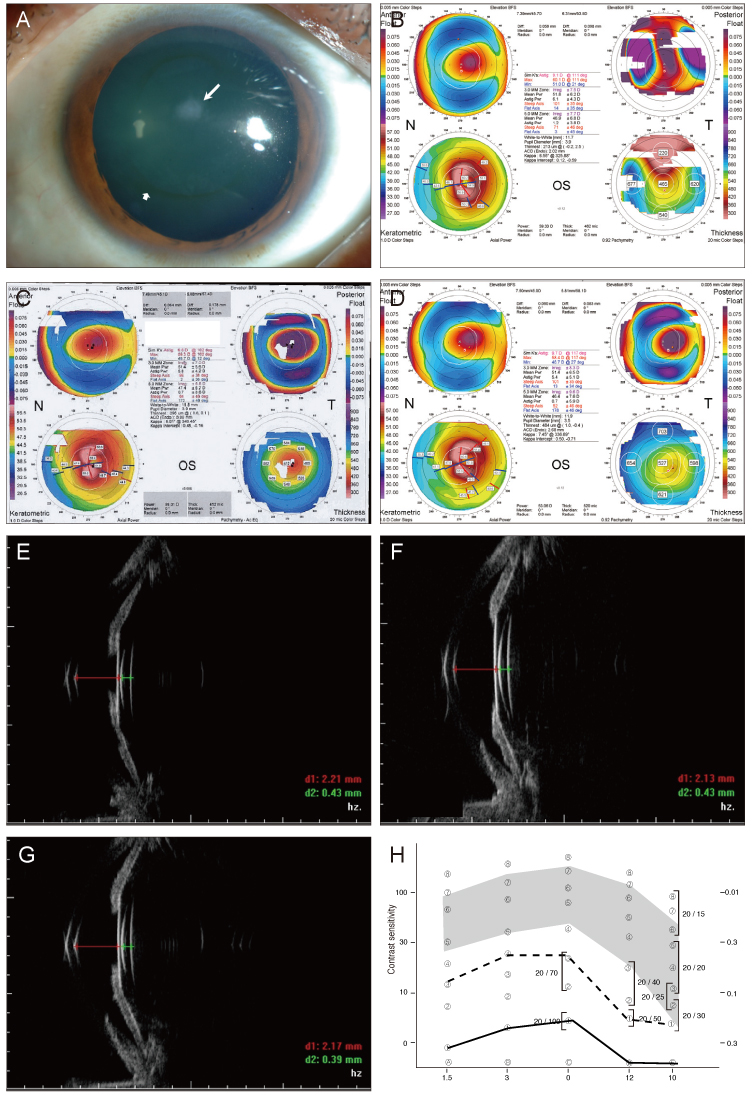
Fig. 1 (A) Anterior segment photography, arrow marking Fleischer's ring, ar rowhead marking corneal scarring. (B) Topography taken 7 years before surgery. (C) Topography before surgery shows stable keratoconus compared with Fig. 1B. The preoperative 3 mm zone irregular astigmatism was ±8.3 diopters and the central corneal thickness was 527 µm. (D) Topography taken 9 months after surgery shows stable keratoconus compared with preoperative topographies. (E) The ultrasound biomicroscopy (UBM) measurement of anterior chamber depth from the endothelium to the anterior surface of implantable collamer lens (ICL) was 2.21 mm one month after surgery. (F) The UBM measurement of anterior chamber depth from the endothelium to the anterior surface of ICL was 2.13 mm 9 months after surgery. (G) The UBM measurement of anterior chamber depth from the endothelium to the anterior surface of ICL was 2.17 mm 20 months after surgery. (H) Contrast sensitivity improved after toric ICL implantation (solid line, postoperative 1 month; dashed line, postoperative 9 months).
Reference
-
1. Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984. 28:293–322.2. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998. 42:297–319.3. Tuft SJ, Moodaley LC, Gregory WM, et al. Prognostic factors for the progression of keratoconus. Ophthalmology. 1994. 101:439–447.4. Lass JH, Lembach RG, Park SB, et al. Clinical management of keratoconus: a multicenter analysis. Ophthalmology. 1990. 97:433–445.5. Brierly SC, Izquierdo L Jr, Mannis MJ. Penetrating keratoplasty for keratoconus. Cornea. 2000. 19:329–332.6. Sekundo W, Stevens JD. Surgical treatment of keratoconus at the turn of the 20th century. J Refract Surg. 2001. 17:69–73.7. Jhanji V, Sharma N, Vajpayee RB. Management of keratoconus: current scenario. Br J Ophthalmol. 2011. 95:1044–1050.8. Kubaloglu A, Cinar Y, Sari ES, et al. Comparison of 2 intrastromal corneal ring segment models in the management of keratoconus. J Cataract Refract Surg. 2010. 36:978–985.9. Colin J, Malet FJ. Intacs for the correction of keratoconus: two-year follow-up. J Cataract Refract Surg. 2007. 33:69–74.10. Rabinowitz YS. INTACS for keratoconus. Int Ophthalmol Clin. 2010. 50:63–76.11. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003. 135:620–627.12. Sanders DR, Schneider D, Martin R, et al. Toric implantable collamer lens for moderate to high myopic astigmatism. Ophthalmology. 2007. 114:54–61.13. Chang J, Lau S. Toric implantable collamer lens for high myopic astigmatic Asian eyes. Ophthalmology. 2009. 116:2340–2347.14. Kamiya K, Shimizu K, Aizawa D, et al. One-year follow-up of posterior chamber toric phakic intraocular lens implantation for moderate to high myopic astigmatism. Ophthalmology. 2010. 117:2287–2294.15. Kamiya K, Shimizu K, Ando W, et al. Phakic toric implantable collamer lens implantation for the correction of high myopic astigmatism in eyes with keratoconus. J Refract Surg. 2008. 24:840–842.16. Gazieva L, Beer MH, Nielsen K, Hjortdal J. A retrospective comparison of efficacy and safety of 680 consecutive lasik treatments for high myopia performed with two generations of flying-spot excimer lasers. Acta Ophthalmol. 2011. 89:729–733.17. Sarver EJ, Sanders DR. Astigmatic power calculations for intraocular lenses in the phakic and aphakic eye. J Refract Surg. 2004. 20:472–477.18. Moshirfar M, Feilmeier MR, Kang PC. Implantation of verisyse phakic intraocular lens to correct myopic refractive error after penetrating keratoplasty in pseudophakic eyes. Cornea. 2006. 25:107–111.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rotational Stability after Toric Implantable Collamer Lens Implantation
- Clinical Outcomes of Toric Implantable Collamer Lens implantation
- Short-term Clinical Outcomes of Implantable Collamer Lens Implantation with Simultaneous Full Thickness Astigmatic Keratotomy
- Correction of Internal Astigmatism Using Toric Scleral Contact Lens after Implantable Collamer Lens Surgery
- Sudden Loss of Endothelial Cell Density 7 Years after Receiving an Implantable Contact Lens: A Case Report
