Clinical Demographics and Outcomes in Mechanically Ventilated Patients in Korean Intensive Care Units
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. suhgy@skku.edu
- 2Department of Internal Medicine, College of Medicine, Chungbuk National University School of Medicine, Cheongju, Korea.
- 3Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Yonsei University College of Medicine, Yonsei University Health System, Seoul, Korea.
- 4Department of Internal Medicine, School of Medicine, Ewha Woman's University, Seoul, Korea.
- 5Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Internal Medicine, Hallym University Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea.
- 6Division of Pulmonary, Sleep and Critical Care Medicine, Department of Internal Medicine, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, Korea.
- 7Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 8Department of Internal Medicine, Dongguk University Gyeongju Hospital, Dongguk University College of Medicine, Gyeongju, Korea.
- 9Department of Internal Medicine, Catholic University of Daegu Hospital, Daegu, Korea.
- 10Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Yonsei University Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea.
- 11Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 1796952
- DOI: http://doi.org/10.3346/jkms.2014.29.6.864
Abstract
- Knowledge of clinical demographics and outcomes of mechanically ventilated patients is important but there are few prospectively collected data in Korea. The objective of the present study was to describe the current status of mechanically ventilated patients in Korea as of 2010. We analyzed the data of Korean patients (275 patients in 12 Korean intensive care units [ICU]) participating in a multinational prospective cohort study on mechanical ventilation. The most common indication for mechanical ventilation was pneumonia (23%). Pressure-limited ventilation modes were preferred over volume-cycled ventilation modes. Non-invasive positive pressure ventilation was used in only seven (2%) patients as the initial ventilatory support. Median duration of mechanical ventilation was 7 days and ICU mortality was 36%. The multiple logistic regression model revealed that the Simplified Acute Physiology Score II (SAPS II) score at ICU admission (odds ratio [OR], 1.034; 95% confidence interval [CI], 1.001-1.036; P=0.033), peak pressure (OR, 1.054; 95% CI, 1.016-1.095; P=0.006), and the number of failed organs (OR, 2.132; 95% CI, 1.634-2.781; P<0.001) were independently associated with ICU mortality. This study provides a snapshot of current practice of mechanical ventilation in Korea.
Keyword
MeSH Terms
-
Acute Disease
Aged
Cohort Studies
Demography
Female
Hospital Mortality
Humans
Intensive Care Units/*statistics & numerical data
Length of Stay
Male
Middle Aged
Odds Ratio
Prognosis
Prospective Studies
Republic of Korea
*Respiration, Artificial
Respiratory Insufficiency/*diagnosis/epidemiology/mortality
Sepsis/etiology
Severity of Illness Index
Figure
-
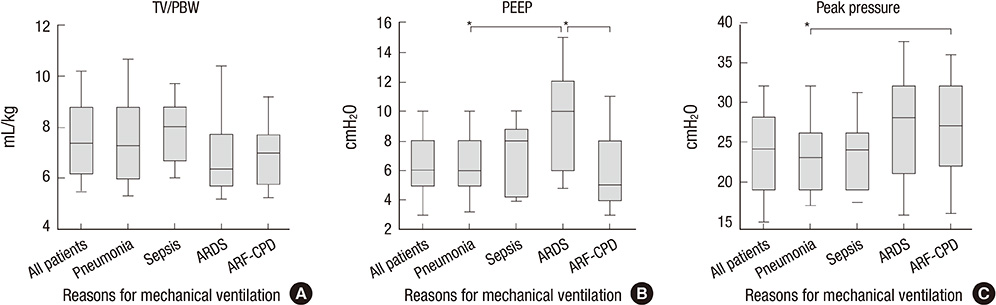
Fig. 1 Initial settings of ventilator according to reason for initiating mechanical ventilation. Boxes indicate interquartile ranges and whiskers indicate 10 to 90 percentile ranges. *P<0.05 by Bonferroni adjusted Mann-Whitney U-test. TV, tidal volume; PBW, predicted body weight; PEEP, positive end-expiratory pressure; ARDS, acute respiratory distress syndrome; ARF-CPD, acute respiratory failure on chronic pulmonary disease.
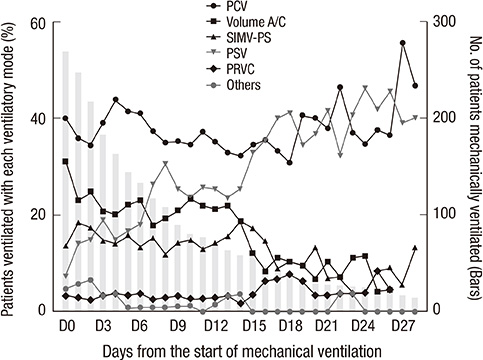
Fig. 2 Ventilator modes used each day during the course of mechanical ventilation. Bar graphs indicate the total number of patients who received mechanical ventilation by days from the start of mechanical ventilation. Lines indicate the percentage of ventilatory mode by each day, respectively. PCV, pressure control ventilation; A/C, assist/control mode; SIMV-PS, synchronized intermittent mandatory ventilation with pressure support; PSV, pressure support ventilation; PRVC, pressure regulated volume control.
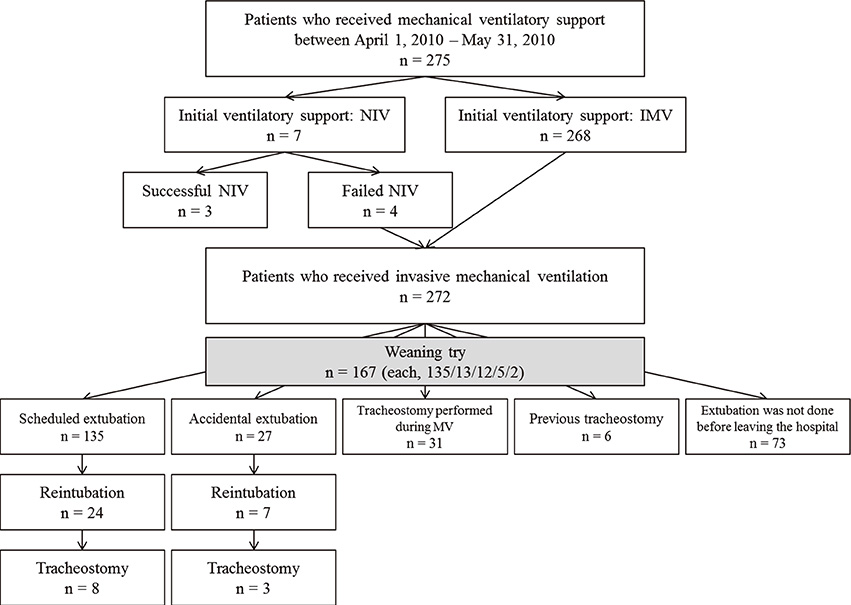
Fig. 3 Clinical course of patients who received mechanical ventilator support. NIV, non-invasive ventilator; IMV, invasive mechanical ventilator; MV, mechanical ventilation.
Cited by 1 articles
-
Association between mechanical power and intensive care unit mortality in Korean patients under pressure-controlled ventilation
Jae Kyeom Sim, Sang-Min Lee, Hyung Koo Kang, Kyung Chan Kim, Young Sam Kim, Yun Seong Kim, Won-Yeon Lee, Sunghoon Park, So Young Park, Ju-Hee Park, Yun Su Sim, Kwangha Lee, Yeon Joo Lee, Jin Hwa Lee, Heung Bum Lee, Chae-Man Lim, Won-Il Choi, Ji Young Hong, Won Jun Song, Gee Young Suh
Acute Crit Care. 2024;39(1):91-99. doi: 10.4266/acc.2023.00871.
Reference
-
1. Esteban A, Anzueto A, Frutos F, Alía I, Brochard L, Stewart TE, Benito S, Epstein SK, Apezteguía C, Nightingale P, et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002; 287:345–355.2. Esteban A, Ferguson ND, Meade MO, Frutos-Vivar F, Apezteguia C, Brochard L, Raymondos K, Nin N, Hurtado J, Tomicic V, et al. Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med. 2008; 177:170–177.3. Esteban A, Frutos-Vivar F, Muriel A, Ferguson ND, Peñuelas O, Abraira V, Raymondos K, Rios F, Nin N, Apezteguía C, et al. Evolution of mortality over time in patients receiving mechanical ventilation. Am J Respir Crit Care Med. 2013; 188:220–230.4. Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. 2010; 38:1947–1953.5. Hong SB, Oh BJ, Kim YS, Kang EH, Kim CH, Park YB, Han MS, Shin C. the Korean Study Group on Respiratory Failure (KOSREF). Characteristics of mechanical ventilation employed in intensive care units: a Multicenter Survey of Hospitals. J Korean Med Sci. 2008; 23:948–953.6. Koh Y, Lim CM, Koh SO, Ahn JJ, Kim YS, Jung BH, Cho JH, Lee JH, Lee MG, Jung KS, et al. A national survey on the practice and outcomes of mechanical ventilation in Korean intensive care units. Anaesth Intensive Care. 2009; 37:272–280.7. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis: the ACCP/SCCM Consensus Conference Committee: American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992; 101:1644–1655.8. Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Legall JR, Morris A, Spragg R. The American-European Consensus Conference on ARDS: definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994; 149:818–824.9. Garner JS, Jarvis WR, Emori TG, Horan TC, Hughes JM. CDC definitions for nosocomial infections, 1988. Am J Infect Control. 1988; 16:128–140.10. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure: on behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996; 22:707–710.11. Plant PK, Owen JL, Elliott MW. Early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre randomised controlled trial. Lancet. 2000; 355:1931–1935.12. Peter JV, Moran JL, Phillips-Hughes J, Graham P, Bersten AD. Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-analysis. Lancet. 2006; 367:1155–1163.13. Hilbert G, Gruson D, Vargas F, Valentino R, Gbikpi-Benissan G, Dupon M, Reiffers J, Cardinaud JP. Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure. N Engl J Med. 2001; 344:481–487.14. Jang HJ, Ra SW, Oh BJ, Lim CM, Koh Y, Hong SB. Korean Study Group on Respiratory Failure (KOSREF). Multicenter prospective observational study about the usage patterns of sedatives, analgesics and neuromuscular blocking agents in the patients requiring more than 72 hours mechanical ventilation in intensive care units of Korea. Korean J Crit Care Med. 2009; 24:145–151.15. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome: the Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000; 342:1301–1308.16. Villar J, Kacmarek RM, Pérez-Méndez L, Aguirre-Jaime A. A high positive end-expiratory pressure, low tidal volume ventilatory strategy improves outcome in persistent acute respiratory distress syndrome: a randomized, controlled trial. Crit Care Med. 2006; 34:1311–1318.17. Park G, Lane M, Rogers S, Bassett P. A comparison of hypnotic and analgesic based sedation in a general intensive care unit. Br J Anaesth. 2007; 98:76–82.18. Breen D, Karabinis A, Malbrain M, Morais R, Albrecht S, Jarnvig IL, Parkinson P, Kirkham AJ. Decreased duration of mechanical ventilation when comparing analgesia-based sedation using remifentanil with standard hypnotic-based sedation for up to 10 days in intensive care unit patients: a randomised trial [ISRCTN47583497]. Crit Care. 2005; 9:R200–R210.19. Hermans G, De Jonghe B, Bruyninckx F, Van den Berghe G. Clinical review: critical illness polyneuropathy and myopathy. Crit Care. 2008; 12:238.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of salivary and serum cortisol levels in mechanically ventilated patients and non-critically ill patients
- Theoretical definition of nurse–conscious mechanically ventilated patient communication: a scoping review with qualitative content analysis
- Management of Pain, Agitation and Delirium in the Intensive Care Units
- Rehabilitation in Intensive Care Unit
- Incidence of Colonization, Ventilator-Associated Pneumonia as Related to the Type of Endotracheal Suction System in Mechanically Ventilated Patients
