Ophthalmic Artery Aneurysm: Potential Culprit of Central Retinal Artery Occlusion
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Ophthalmology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. sejoon1@snu.ac.kr
- 3Department of Ophthalmology, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Neurosurgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- KMID: 1792086
- DOI: http://doi.org/10.3341/kjo.2013.27.6.470
Abstract
- Central retinal artery occlusion (CRAO) is one of the most devastating ophthalmic emergencies, causing acute painless visual loss in the affected eye. We describe the first case of acute non-arteritic CRAO associated with peripheral ophthalmic artery aneurysm and its clinical course after intra-arterial thrombolysis therapy. This case suggests that ophthalmic artery aneurysm can be the cause of CRAO and should be included in the differential diagnosis of CRAO.
MeSH Terms
Figure
-
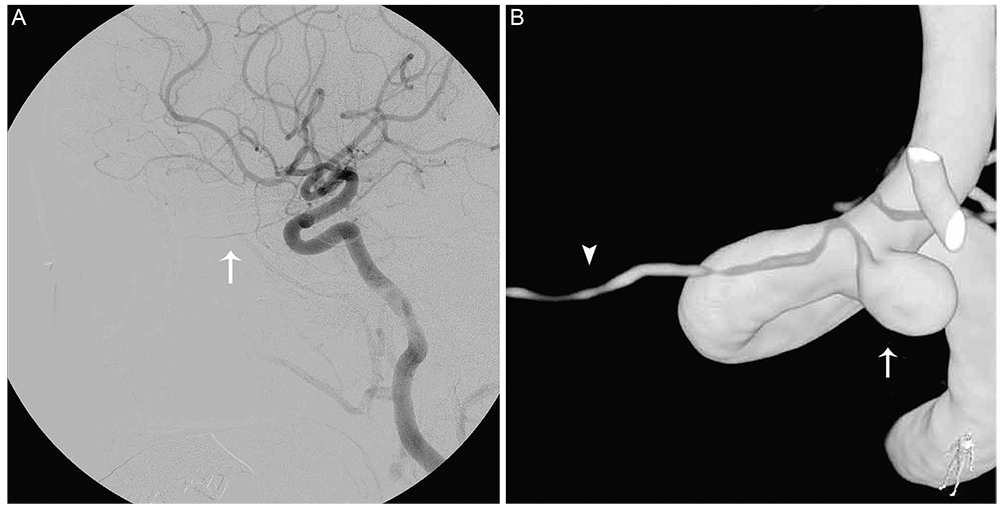
Fig. 1 Internal carotid artery angiogram and three dimensional reconstructed image of the ophthalmic artery. (A) The internal carotid artery angiogram shows patent ophthalmic artery (arrow). (B) Three dimensional reconstructed view of the ophthalmic artery (arrow head) identifies its origin from the 3.7 × 4.5 × 5.2 mm sized aneurysm (arrow).
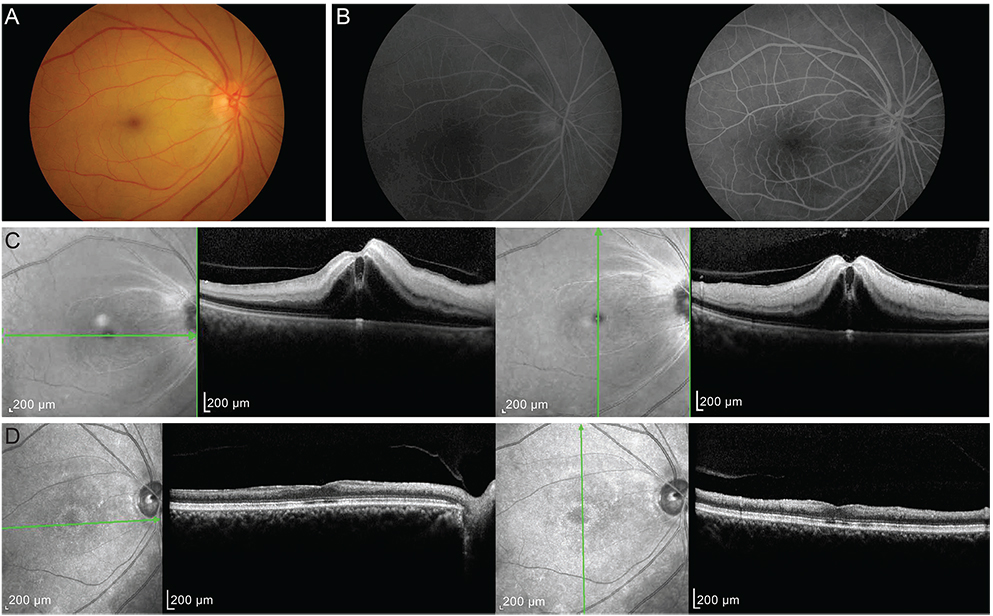
Fig. 2 Fundus photography, fluorescein angiography and spectral-domain optical coherence tomography (SD-OCT) after intra-arterial thrombolysis. (A) One day after thrombolysis, the retina was still edematous with a typical "cherry red spot" appearance but showed improved vascularity. (B) Retinal arterial filling showed normal arterio-venous transit time of 11 seconds (left 20 seconds, right 31 seconds). (C) SD-OCT showed increased thickness and reflectivity of the inner retina typical of central retinal artery occlusion. (D) After 4 months of treatment, the inner retina thickness had markedly decreased.
Reference
-
1. Rumelt S, Dorenboim Y, Rehany U. Aggressive systematic treatment for central retinal artery occlusion. Am J Ophthalmol. 1999; 128:733–738.2. Hayreh SS, Podhajsky PA, Zimmerman MB. Retinal artery occlusion: associated systemic and ophthalmic abnormalities. Ophthalmology. 2009; 116:1928–1936.3. Qiao L, Wang H, Mao L, et al. Peripheral ophthalmic artery aneurysm. Neurosurg Rev. 2011; 34:29–38.4. Qureshi AI, Mohammad Y, Yahia AM, et al. Ischemic events associated with unruptured intracranial aneurysms: multicenter clinical study and review of the literature. Neurosurgery. 2000; 46:282–289.5. Haritoglou C, Muller-Schunk S, Weber C, et al. Central retinal artery occlusion in association with an aneurysm of the internal carotid artery. Am J Ophthalmol. 2001; 132:270–271.6. Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: a statement for healthcare professionals from the Stroke Council of the American Heart Association. Circulation. 2000; 102:2300–2308.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Incomplete Central Retinal Artery Occlusion
- Intra-arterial Thrombolysis for Central Retinal Artery Occlusion after the Coil Embolization of Paraclinoid Aneurysm
- Central Retinal Artery Occlusion Masquerading as Branch Retinal Artery Occlusion
- Embolization through the Ophthalmic Artery with Onyx in Bilateral Ethmoidal Dural Arteriovenous Fistula: A Case Report
- The Successful Treatment of a Case of Central Retinal Artery Occlusion
