Biologic Fixation through Bridge Plating for Comminuted Shaft Fracture of the Clavicle: Technical Aspects and Prospective Clinical Experience with a Minimum of 12-Month Follow-up
- Affiliations
-
- 1Department of Orthopaedic Surgery, Kosin University Gospel Hospital, Busan, Korea. jyujin2001@kosin.ac.kr
- 2Department of Trauma Surgery, Kosin University Gospel Hospital, Busan, Korea.
- KMID: 1787037
- DOI: http://doi.org/10.4055/cios.2013.5.4.327
Abstract
- For comminuted shaft fracture of clavicle, the operative goal, aside from sound bone healing without complications of direct reduction, is maintenance of the original length in order to maintain the normal biomechanics of adjacent joint. Our bridge plating technique utilizing distraction through a lumbar spreader was expected to be effective for restoring clavicular length with soft tissue preservation. However, there are two disadvantages. First, there is more exposure to radiation compared to conventional plating; and second, it is difficult to control the rotational alignment. Despite these disadvantages, our technique has important benefits, in particular, the ability to preserve clavicular length without soft tissue injury around the fracture site.
MeSH Terms
Figure
-

Fig. 1 A 20-year-old woman injured in a sports accident (Judo). Simple radiographs showed a comminuted segmental fracture of the clavicle (Robinson classification, 2B2).
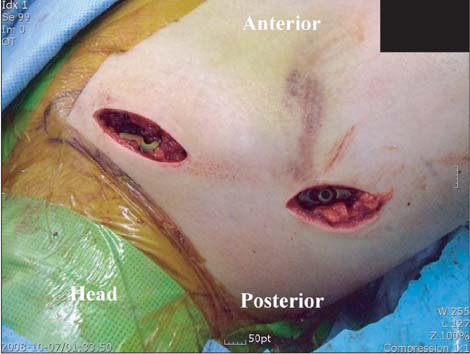
Fig. 2 The fracture was fixed by biologic fixation through bridge plating to preserve the soft tissue around the fracture site.
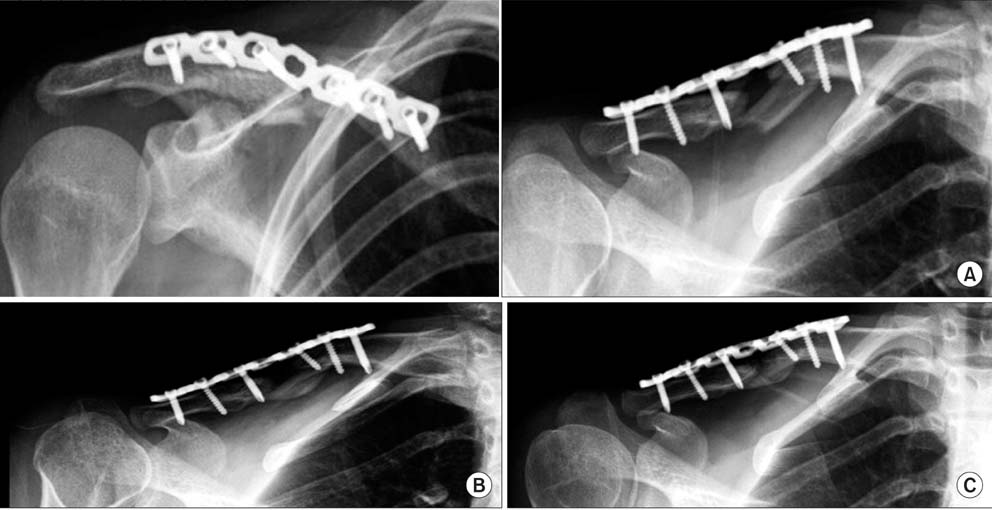
Fig. 3 (A) Postoperatively, the fractured clavicle failed to achieve cortical contact due to indirect reduction. (B) Callus bridging occurred 16 weeks after surgery. (C) The clavicle was remodeled at 9 months follow-up.

Fig. 4 The shoulder motion was fully recovered to the preinjury level.
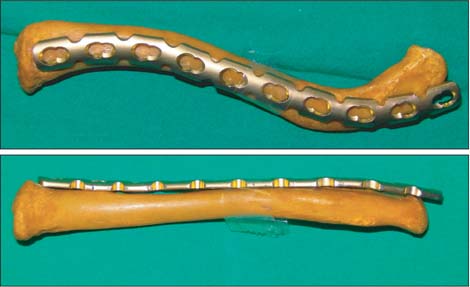
Fig. 5 A locking reconstruction plate (Synthes) was preoperatively bent to match the normal cadaveric clavicle.
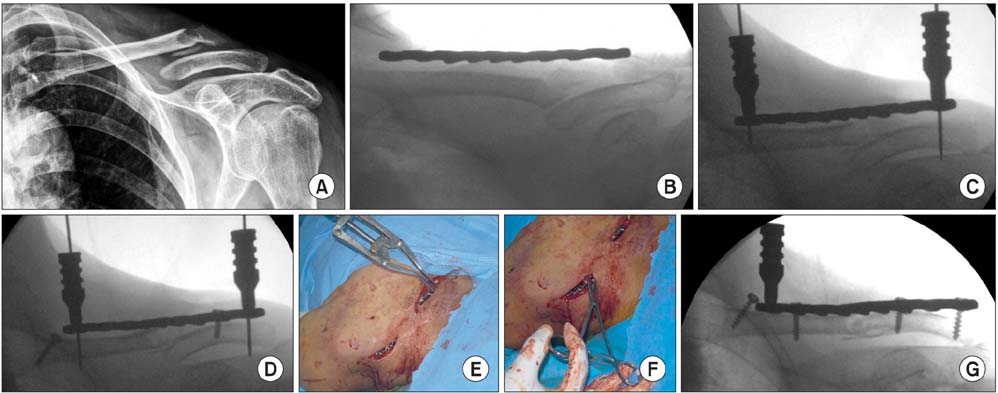
Fig. 6 Stepwise reduction and fixation. (A) Simple radiograph shows clavicular fracture with comminution and shortening, and the overlapping fragments. (B, C) The plate was passed through a submuscular tunnel and provisionally fixed with K-wires. (D) After fixation of the shorter fragment with a conventional screw, distractive force was applied through a lumbar spreader to achieve ligamentotaxis with the K-wire. (E and F) Simulated photos show how to use the lumbar spreader and Kelly clamp for indirect reduction. (G) The realignment of fracture sites was achieved by indirect reduction.

Fig. 7 Postoperative radiographs show the restoration of clavicular length and realignment of comminuted segments.
Cited by 1 articles
-
A Comparison between Open Reduction/Internal Fixation and Minimally Invasive Plate Osteosynthesis Using a 3-Dimensional Printing Model for Displaced Clavicular Fractures
Dong-Soo Kim, Ho-Seung Jeong, Kyoung-Jin Park, Hyun-Chul Shon, Jae-Young Yang
J Korean Orthop Assoc. 2018;53(4):324-331. doi: 10.4055/jkoa.2018.53.4.324.
Reference
-
1. Canale ST, Beaty JH. Campbell's operative orthopaedics. 11th ed. Philadelphia: Mosby;2007. p. 3371–3376.2. Wijdicks FJ, Van der Meijden OA, Millett PJ, Verleisdonk EJ, Houwert RM. Systematic review of the complications of plate fixation of clavicle fractures. Arch Orthop Trauma Surg. 2012; 132(5):617–625.3. Martinez AA, Cuenca J, Herrera A. Philos plate fixation for proximal humeral fractures. J Orthop Surg (Hong Kong). 2009; 17(1):10–14.4. Nowak J, Holgersson M, Larsson S. Can we predict long-term sequelae after fractures of the clavicle based on initial findings? A prospective study with nine to ten years of follow-up. J Shoulder Elbow Surg. 2004; 13(5):479–486.5. Khan LA, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg Am. 2009; 91(2):447–460.6. Krettek C, Muller M, Miclau T. Evolution of minimally invasive plate osteosynthesis (MIPO) in the femur. Injury. 2001; 32:Suppl 3. SC14–SC23.7. Smekal V, Oberladstaetter J, Struve P, Krappinger D. Shaft fractures of the clavicle: current concepts. Arch Orthop Trauma Surg. 2009; 129(6):807–815.8. Robertson C, Celestre P, Mahar A, Schwartz A. Reconstruction plates for stabilization of mid-shaft clavicle fractures: differences between nonlocked and locked plates in two different positions. J Shoulder Elbow Surg. 2009; 18(2):204–209.9. Liu PC, Chien SH, Chen JC, Hsieh CH, Chou PH, Lu CC. Minimally invasive fixation of displaced midclavicular fractures with titanium elastic nails. J Orthop Trauma. 2010; 24(4):217–223.10. Huang JI, Toogood P, Chen MR, Wilber JH, Cooperman DR. Clavicular anatomy and the applicability of precontoured plates. J Bone Joint Surg Am. 2007; 89(10):2260–2265.11. Andermahr J, Jubel A, Elsner A, et al. Anatomy of the clavicle and the intramedullary nailing of midclavicular fractures. Clin Anat. 2007; 20(1):48–56.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Does Interfragmentary Cerclage Wire Fixation in Clavicle Shaft Fracture Interfere the Fracture Healing?
- Additional fixation using a metal plate with bioresorbable screws and wires for robinson type 2B clavicle fracture
- Use of Composite Wiring on Surgical Treatments of Clavicle Shaft Fractures
- Intramedullary Fixation in the Fracture of the Shaft of the Clavicle by Threaded Kirschner Wire
- Surgical Techniques for Percutaneous Reduction by Towel Clips and Percutaneous Intramedullary Fixation with Steinmann Pins for Clavicle Shaft Fractures
