Electrode Position and the Clinical Outcome after Bilateral Subthalamic Nucleus Stimulation
- Affiliations
-
- 1Movement Disorder Center and Clinical Research Institute, Seoul National University Hospital, Seoul, Korea. brain@snu.ac.kr
- 2Department of Neurosurgery, Seoul National University Hospital, Seoul, Korea.
- 3Department of Neurology, Seoul National University Hospital, Seoul, Korea.
- 4Department of Preventive Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 5Neuroscience Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- 6Ischemia Hypoxia Disease Institute, Seoul National University College of Medicine, Seoul, Korea.
- 7Cancer Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- 83D Medical Imaging Lab, CyberMed, Seoul, Korea.
- KMID: 1785994
- DOI: http://doi.org/10.3346/jkms.2011.26.10.1344
Abstract
- We compared the surgical outcome with electrode positions after bilateral subthalamic nucleus (STN) stimulation surgery for Parkinson's disease. Fifty-seven patients treated with bilateral STN stimulations were included in this study. Electrode positions were determined in the fused images of preoperative MRI and postoperative CT taken at six months after surgery. The patients were divided into three groups: group I, both electrodes in the STN; group II, only one electrode in the STN; group III, neither electrode in the STN. Unified Parkinson's Disease Rating Scale (UPDRS), Hoehn and Yahr stage, and activities of daily living scores significantly improved at 6 and 12 months after STN stimulation in both group I and II. The off-time UPDRS III speech subscore significantly improved (1.6 +/- 0.7 at baseline vs 1.3 +/- 0.8 at 6 and 12 months, P < 0.01) with least L-dopa equivalent daily dose (LEDD) (844.6 +/- 364.1 mg/day at baseline; 279.4 +/- 274.6 mg/day at 6 months; and 276.0 +/- 301.6 mg/day at 12 months, P < 0.001) at 6 and 12 months after STN deep brain stimulation (DBS) in the group I. Our findings suggest that the better symptom relief including speech with a reduced LEDD is expected in the patients whose electrodes are accurately positioned in both STN.
Keyword
MeSH Terms
-
Adult
Aged
Antiparkinson Agents/adverse effects/*therapeutic use
Combined Modality Therapy
*Deep Brain Stimulation/adverse effects/instrumentation/methods
*Electrodes, Implanted
Female
Humans
Levodopa/adverse effects/therapeutic use
Magnetic Resonance Imaging
Male
Middle Aged
Parkinson Disease/drug therapy/*therapy
Severity of Illness Index
Subthalamic Nucleus/*physiology
Treatment Outcome
Figure
-
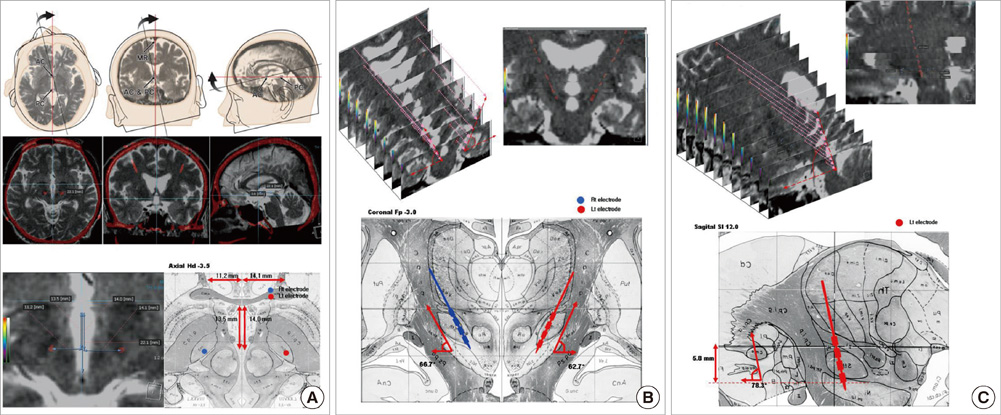
Fig. 1 Fused images of the preoperative MRI and postoperative CT. The T2-weighted axial images of brain MRI taken before surgery are fused with 3-D spiral CT scan images at the data set of 1-mm thickness reformatted images, aligned to anterior commissure - posterior commissure (AC-PC) line. The midline of reformatted coronal images also intersect the midsagittal plane for the correction of head-rotation error. The length of AC-PC line and width of the third ventricle are taken into consideration for the proportional localization of the electrodes position in the human brain atlas of Schaltenbrad and Wahren. In the reformatted axial images the lateral distance from the midline and the anteroposterior distance from the mid-commissural line to each electrode are measured (A). In the reformatted coronal images in which the electrode trajectory is best visualized, the lateral angles of the electrode trajectory from the midline are measured for each electrode in every patient (B). In the reformatted sagittal images in which the electrode trajectory is best shown, the antero-posterior angle of the electrode trajectory from the line perpendicular to the AC-PC line and the depth of the electrodes are also measured for each electrode in every patient (C).
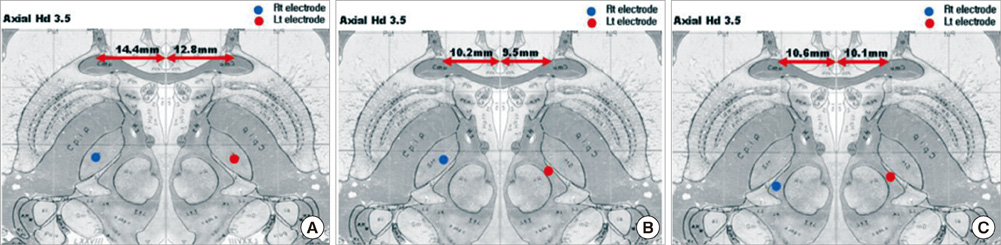
Fig. 2 Plotting of electrode positions in the human brain atlas. With the information from the fused images of preoperative MRI and postoperative CT taken at 6 months after surgery as shown in Fig. 1, the electrode positions are plotted on the human brain atlas of Schaltenbrand and Wahren in each patient. Representative illustration of the electrode positions (A-C) are plotted in the axial, sagittal, and coronal planes. Based on the axial view at the level of 3.5 mm below the AC-PC line in the atlas, electrode positions (in blue and red colors) are categorized into three groups: 1) group I, both electrodes in the STN (n = 36) (A); 2) group II, only one electrode in the STN (n = 16) (B); 3) group III, neither electrode in the STN (n = 5) (C).
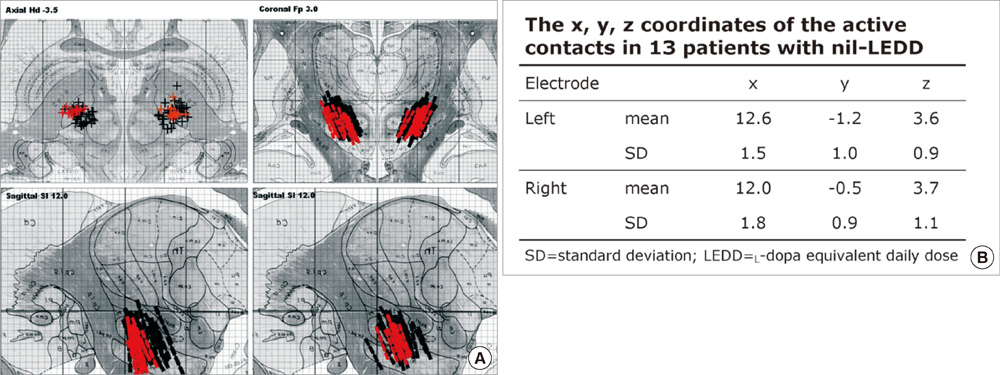
Fig. 3 Electrode positions of 13 patients without medication after surgery. (A) The location of the electrodes are plotted based on the fused images of the 13 patients showing significant clinical improvement in UPDRS part III including speech with nil LEDD (in red color) and of the remaining 44 patients (in black color) at the last follow-up period of more than one year after surgery. Most electrodes of these 13 patients are positioned in the middle one third of the subthalamic nucleus in the axial view at the level of 3.5 mm below the AC-PC line (upper left), and also positioned in the subthalamic nucleus in the coronal view at the level of 3.0 mm posterior to midcommissural point (upper right) and in the sagittal view at the level of 12 mm lateral to the midline (lower). (B) The x, y, z coordinates of the active contacts referenced to the AC-PC midpoints in the 13 patients with nil LEDD.
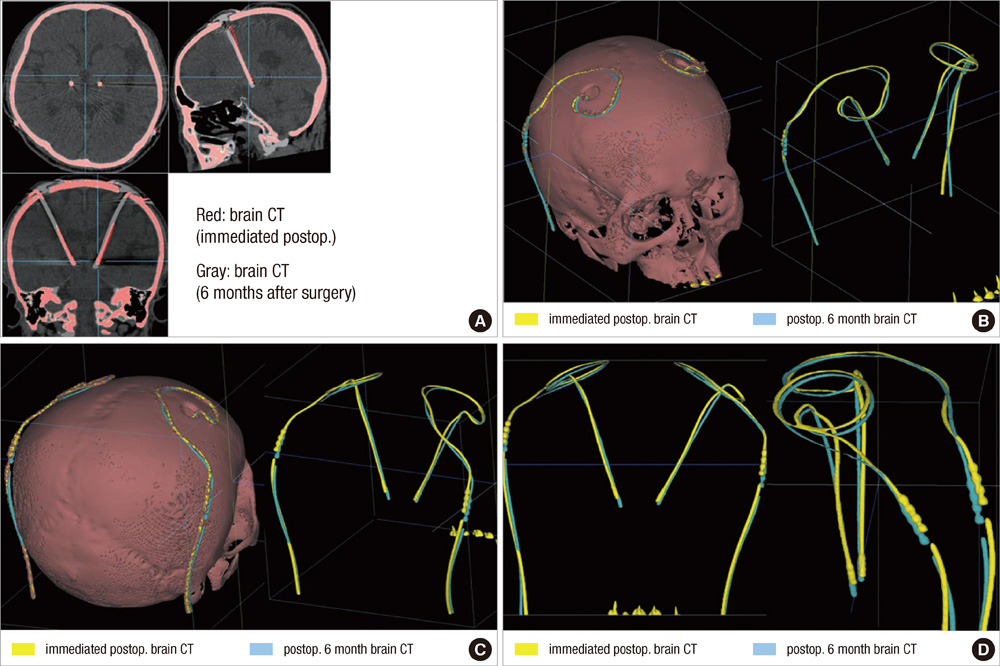
Fig. 4 Fused images of two brain CT scans taken after surgery. The fused images obtained from the CT scans taken at the immediate postoperative day and six months after surgery are aligned along the AC-PC line at the level of AC and PC in axial, sagittal, and coronal plane. The red represents the electrode extracted from the images of brain CT taken immediately after surgery and the gray represents the electrode extracted from the images of the brain CT taken at six months after surgery. The red and the gray electrodes do not fit into each other with significant discrepancy of their position in the axial and coronal planes (A). With the adjustment of window level and width of the fused images, only the shadow of both electrodes is extracted in 3-D reconstructive rendering image of right superior oblique view (B), right posterior oblique view (C), and AP and lateral view (D). The yellow represents the electrode extracted from the images of brain CT taken immediately after surgery and the sky-blue represents the electrode extracted from the images of the brain CT taken at six months after surgery. Significant discrepancy of the electrode position between the two CT scans is remarkable.
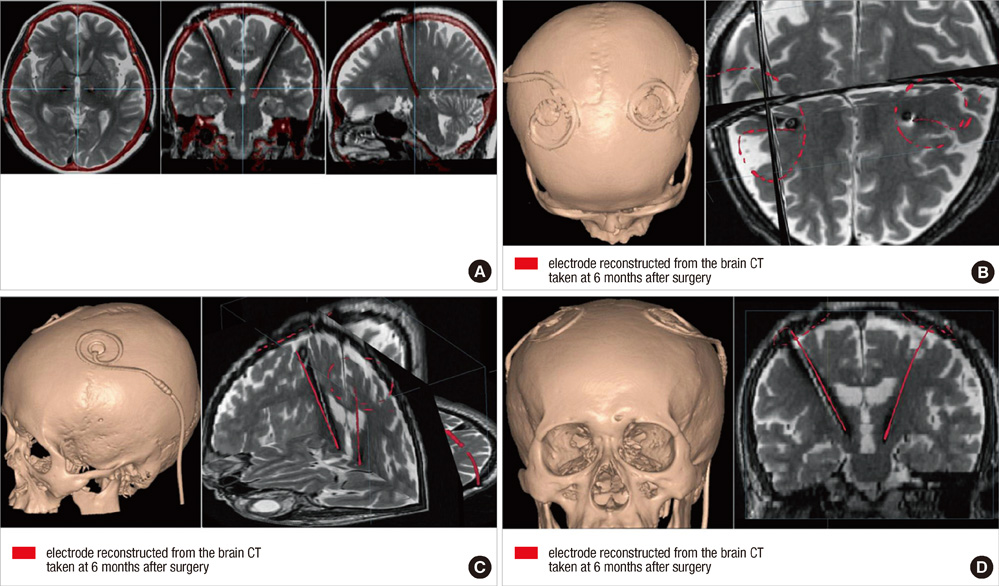
Fig. 5 Fused images of brain CT and MRI taken after surgery. Fused images of the brain CT and the brain MRI both taken at 6 months after bilateral subthalamic stimulation are illustrated. The fused images obtained from the brain MRI and the brain CT taken at 6 months after bilateral subthalamic stimulation are aligned along the AC-PC line at the level of AC and PC in axial, sagittal, and coronal plane. The red represents the electrode extracted from the images of brain CT taken at six months after surgery and the gray represents the electrode extracted from the images of the brain MRI taken at six months after surgery. The center of red and gray one representing the center of electrodes extracted from brain CT and brain MRI do not fit into each other with significant discrepancy of their position in the axial, coronal, and sagittal plane of the fused images (A). With the adjustment of window level and width of the fused images, only the electrodes in red color are superimposed in 3-D reconstructive rendering brain MR images of superior anterior view (B), left anterior superior oblique view (C), and anterior posterior view (D). The discrepancy of the electrode position extracted from brain CT and the center of electrode artifact from brain MRI taken at 6 months after surgery is remarkable in all three axial, sagittal, and coronal planes.
Cited by 1 articles
-
Factors Related to Outcomes of Subthalamic Deep Brain Stimulation in Parkinson's Disease
Hae Yu Kim, Won Seok Chang, Dong Wan Kang, Young Ho Sohn, Myung Sik Lee, Jin Woo Chang
J Korean Neurosurg Soc. 2013;54(2):118-124. doi: 10.3340/jkns.2013.54.2.118.
Reference
-
1. Krack P, Batir A, Van Blercom N, Chabardes S, Fraix V, Ardouin C, Koudsie A, Limousin PD, Benazzouz A, LeBas JF, Benabid AL, Pollak P. Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson's disease. N Engl J Med. 2003. 349:1925–1934.2. Limousin P, Krack P, Pollak P, Benazzouz A, Ardouin C, Hoffmann D, Benabid AL. Electrical stimulation of the subthalamic nucleus in advanced Parkinson's disease. N Engl J Med. 1998. 339:1105–1111.3. Bejjani BP, Dormont D, Pidoux B, Yelnik J, Damier P, Arnulf I, Bonnet AM, Marsault C, Agid Y, Philippon J, Cornu P. Bilateral subthalamic stimulation for Parkinson's disease by using three-dimensional stereotactic magnetic resonance imaging and electrophysiological guidance. J Neurosurg. 2000. 92:615–625.4. Godinho F, Thobois S, Magnin M, Guenot M, Polo G, Benatru I, Xie J, Salvetti A, Garcia-Larrea L, Broussolle E, Mertens P. Subthalamic nucleus stimulation in Parkinson's disease: anatomical and electrophysiological localization of active contacts. J Neurol. 2006. 253:1347–1355.5. Lanotte MM, Rizzone M, Bergamasco B, Faccani G, Melcarne A, Lopiano L. Deep brain stimulation of the subthalamic nucleus: anatomical and neurophysiological and outcome correlations with the effects of stimulation. J Neurol Neurosurg Psychiatry. 2002. 72:53–58.6. Saint-Cyr JA, Hoque T, Pereira LC, Dostrovsky JO, Hutchison WD, Mikulis DJ, Abosch A, Sime E, Lang AE, Lozano AM. Localization of clinically effective stimulating electrodes in the human subthalamic nucleus on magnetic resonance imaging. J Neurosurg. 2002. 97:1152–1166.7. Yelnik J, Damier P, Demeret S, Gervais D, Bardinet E, Bejjani BP, François C, Houeto JL, Arnule I, Dormont D, Galanaud D, Pidoux B, Cornu P, Agid Y. Localization of stimulating electrodes in patients with Parkinson disease by using a three-dimensional atlas-magnetic resonance imaging coregistration method. J Neurosurg. 2003. 99:89–99.8. Halpern CH, Danish SF, Baltuch GH, Jaggi JL. Brain shift during deep brain stimulation surgery for Parkinson's disease. Stereotact Funct Neurosurg. 2008. 86:37–43.9. Khan MF, Mewes K, Gross RE, Skrinjar O. Assessment of brain shift related to deep brain stimulation surgery. Stereotact Funct Neurosurg. 2008. 86:44–53.10. Miyagi Y, Shima F, Sasaki T. Brain shift: an error factor during implantation of deep brain stimulation electrodes. J Neurosurg. 2007. 107:989–997.11. Martinez-Santiesteban FM, Swanson SD, Noll DC, Anderson DJ. Magnetic field perturbation of neural recording and stimulating microelectrodes. Phys Med Biol. 2007. 52:2073–2088.12. Paek SH, Han JH, Lee JY, Kim C, Jeon BS, Kim DG. Electrode position determined by fused images of preoperative and postoperative magnetic resonance imaging and surgical outcome after subthalamic nucleus deep brain stimulation. Neurosurgery. 2008. 63:925–936.13. Heo JH, Lee KM, Paek SH, Kim MJ, Lee JY, Kim JY, Cho SY, Lim YH, Kim MR, Jeong SY, Jeon BS. The effects of bilateral subthalamic nucleus deep brain stimulation (STN DBS) on cognition in Parkinson disease. J Neurol Sci. 2008. 273:19–24.14. Christensen GE, Joshi SC, Miller MI. Volumetric transformation of brain anatomy. IEEE Trans Med Imaging. 1997. 16:864–877.15. Ferroli P, Franzini A, Marras C, Maccagnano E, D'Incerti L, Broggi G. A simple method to assess accuracy of deep brain stimulation electrode placement: pre-operative stereotactic CT+ postoperative MR image fusion. Stereotact Funct Neurosurg. 2004. 82:14–19.16. Ken S, Di Gennaro G, Giulietti G, Sebastiano F, De Carli D, Garreffa G, Colonnese C, Passariello R, Lotterie JA, Maraviglia B. Quantitative evaluation for brain CT/MRI coregistration based on maximization of mutual information in patients with focal epilepsy investigated with subdural electrodes. Magn Reson Imaging. 2007. 25:883–888.17. Kim HJ, Paek SH, Kim JY, Lee JY, Lim YH, Kim DG, Jeon BS. Two-year follow-up on the effect of unilateral subthalamic deep brain stimulation in highly asymmetric Parkinson's disease. Mov Disord. 2009. 24:329–335.18. Pluim JP, Maintz JB, Viergever MA. Mutual-information-based registration of medical images: a survey. IEEE Trans Med Imaging. 2003. 22:986–1004.19. Schaltenbrand G, Wahren W. Atlas for stereotaxy of the human brain. 1977. 2nd ed. Stuttgart·New York: Thieme.20. Herzog J, Volkmann J, Krack P, Kopper F, Pötter M, Lorenz D, Steinbach M, Klebe S, Hamel W, Schrader B, Weinert D, Müller D, Mehdorn HM, Deuschl G. Two-year follow-up of subthalamic deep brain stimulation in Parkinson's disease. Mov Disord. 2003. 18:1332–1337.21. Coyne T, Silburn P, Cook R, Silberstein P, Mellick G, Sinclair F, Fracchia G, Wasson D, Stanwell P. Rapid subthalamic nucleus deep brain stimulation lead placement utilising CT/MRI fusion, microelectrode recording and test stimulation. Acta Neurochir Suppl. 2006. 99:49–50.22. Duffner F, Schiffbauer H, Breit S, Friese S, Freudenstein D. Relevance of image fusion for target point determination in functional neurosurgery. Acta Neurochir (Wien). 2002. 144:445–451.23. Hamel W, Fietzek U, Morsnowski A, Schrader B, Herzog J, Weinert D, Pfister G, Müller D, Volkmann J, Deuschl G, Mehdorn HM. Deep brain stimulation of the subthalamic nucleus in Parkinson's disease: evaluation of active electrode contacts. J Neurol Neurosurg Psychiatry. 2003. 74:1036–1046.24. Plaha P, Ben-Shlomo Y, Patel NK, Gill SS. Stimulation of the caudal zona incerta is superior to stimulation of the subthatlamic nucleus in improving contralateral parkinsonism. Brain. 2006. 129:1732–1747.25. Voges J, Volkmann J, Allert N, Lehrke R, Koulousakis A, Freund HJ, Sturm V. Bilateral high-frequency stimulation in the subthalamic nucleus for the treatment of Parkinson disease: correlation of therapeutic effect with anatomical electrode position. J Neurosurg. 2002. 96:269–279.26. McClelland S 3rd, Ford B, Senatus PB, Winfield LM, Du YE, Pullman SL, Yu Q, Frucht SJ, McKhann GM 2nd, Goodman RR. Subthalamic stimulation for Parkinson disease: determination of electrode location necessary for clinical efficacy. Neurosurg Focus. 2005. 19:E12.27. Kim YH, Kim HJ, Kim C, Kim DG, Jeon BS, Paek SH. Comparison of electrode location between immediate postoperative day and 6 months after bilateral subthalamic nucleus deep brain stimulation. Acta Neurochir (Wien). 2010. 152:2037–2045.28. Lee JY, Kim JW, Lee JY, Lim YH, Kim C, Kim DG, Jeon BS, Paek SH. Is MRI a reliable tool to locate the electrode after deep brain stimulation surgery? Comparison study of CT and MRI for the localization of electrodes after DBS. Acta Neurochir (Wien). 2010. 152:2029–2036.29. Benabid AL, Chabardès S, Seigneuret E. Deep brain stimulation in Parkinson's disease: long-term efficacy and safety - What happened this year? Curr Opin Neurol. 2005. 18:623–630.30. Pinto S, Thobois S, Costes N, Le Bars D, Benabid AL, Broussolle E, Pollak P, Gentil M. Subthalamic nucleus stimulation and dysarthria in Parkinson's disease: a PET study. Brain. 2004. 127:602–615.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Turning on the Left Side Electrode Changed Depressive State to Manic State in a Parkinson's Disease Patient Who Received Bilateral Subthalamic Nucleus Deep Brain Stimulation: A Case Report
- Deep Brain Stimulation of the Subthalamic and Pedunculopontine Nucleus in a Patient with Parkinson's Disease
- Microelectrode Recording-Guided Deep Brain Stimulation in Patients with Movement Disorders
- The Effect of Bilateral Subthalamic Nucleus Stimulation in Parkinson's Disease: Experiences From 6 Month Follow-up in Sinchon Severance Hospital
- Pilot Study for Considering Subthalamic Nucleus Anatomy during Stimulation Using Directional Leads
