J Korean Med Sci.
2010 Sep;25(9):1394-1397. 10.3346/jkms.2010.25.9.1394.
A Case of Myxedema Coma Presenting as a Brain Stem Infarct in a 74-Year-Old Korean Woman
- Affiliations
-
- 1Department of Emergency Medicine, College of Medicine, Hallym University, Anyang, Korea. medysohn@hallym.or.kr
- 2Department of Emergency Medicine, College of Medicine, Kangwon National University, Chuncheon, Korea.
- KMID: 1785926
- DOI: http://doi.org/10.3346/jkms.2010.25.9.1394
Abstract
- Myxedema coma is the extreme form of untreated hypothyroidism. In reality, few patients present comatose with severe myxedema. We describe a patient with myxedema coma which was initially misdiagnosed as a brain stem infarct. She presented to the hospital with alteration of the mental status, generalized edema, hypothermia, hypoventilation, and hypotension. Initially her brain stem reflexes were absent. After respiratory and circulatory support, her neurologic status was not improved soon. The diagnosis of myxedema coma was often missed or delayed due to various clinical findings and concomitant medical condition and precipitating factors. It is more difficult to diagnose when a patient has no medical history of hypothyroidism. A high index of clinical suspicion can make a timely diagnosis and initiate appropriate treatment. We report this case to alert clinicians considering diagnosis of myxedema coma in patients with severe decompensated metabolic state including mental change.
Keyword
MeSH Terms
Figure
-

Fig. 1 The gross photos of patient's face and extremities. (A, B) Severe periorbital edema and thinned eyebrow. (C, D) Non-pitting edema and desquamation of the hands and feet.

Fig. 2 Initial ECG showed sinus bradycardia (ventricular rate 59/min), low QRS voltage, and a prolonged QT interval (QTc >470 ms).
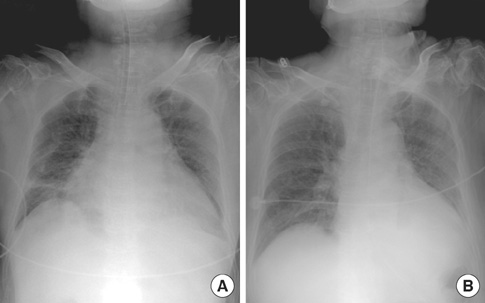
Fig. 3 Chest X-rays. (A) Initial chest X-ray revealed cardiomegaly and infiltration of the left lower lung zone. (B) Follow-up X-ray showed an improved state.
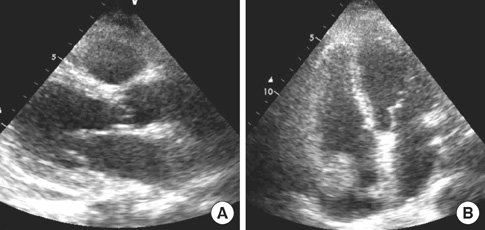
Fig. 4 Echocardiography. Parasternal long axis view (A) and apical four chamber view (B) revealed a moderate amount of pericardial effusion without hemodynamic significance; effusion was localized to the right atrium.
Reference
-
1. Titinalli JE, Kelen GD, Stapczynski JS. Seils A, Fernando N, Watt M, editors. Hypothyroidism and myxedema coma. Emergency Medicine; A comprehensive study guide. 2004. 6th ed. New York: McGraw-Hills Inc;1313–1315.2. Rosen M. Marx J, editor. Hypothyroidism. Rosen's emergency medicine; Concepts and Clinical practice. 2002. 5th ed. St. Louis, MO: Mosby Inc;1774–1779.3. Wall CR. Myxedema coma: diagnosis and treatment. Am Fam Physician. 2000. 62:2485–2490.4. Kwaku MP, Burman KD. Myxedema coma. J Intensive Care Med. 2007. 22:224–231.
Article5. Shim JY, Lee SW, Lee HW, Choi JH, Song YJ, Lee HS, Chung YS, Lee KW. A case of myxedema coma with severe hypoventilation. J Korean Soc Endocrinol. 2004. 19:203–208.6. Rodríguez I, Fluiters E, Pérez-Méndez LF, Luna R, Páramo C, García-Mayor RV. Factors associated with mortality of patients with myxoedema coma: prospective study in 11 cases treated in a single institution. J Endocrinol. 2004. 180:347–350.7. Davis JD, Tremont G. Neuropsychiatric aspects of hypothyroidism and treatment reversibility. Minerva Endocrinol. 2007. 32:49–65.8. Aszalós Z. Some neurologic and psychiatric complications in endocrine disorders: the thyroid gland. Orv Hetil. 2007. 148:303–310.9. Ahn JM, Chun JH, Kwon JW, Park SG, Koh HB, Kim JG. A case of myxedema coma treated with a large oral dose of levothyroxine. Korean J Med. 2009. 76:Suppl 1. S127–S130.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of myxedema coma treated with a large oral dose of levothyroxine
- A Case of Myxedema Coma with Severe Hypoventilation
- Myxedema Coma Successfully Treated by Low Dose Oral Levothyroxine
- A case of rhabdomyolysis developed in patient with thyroid storm
- A case of primary hypothyroidism associated with pretibial myxedema
