J Korean Med Sci.
2008 Aug;23(4):616-620. 10.3346/jkms.2008.23.4.616.
Factors Influencing Residual Pleural Opacity in Tuberculous Pleural Effusion
- Affiliations
-
- 1Department of Internal Medicine and Respiratory Center, Kyungpook National University School of Medicine, Daegu, Korea. sicha@knu.ac.kr
- 2Department of Radiology, Gyeongsang National University School of Medicine, Jinju, Korea.
- KMID: 1785819
- DOI: http://doi.org/10.3346/jkms.2008.23.4.616
Abstract
- Tuberculous pleural effusion (TPE) leads to residual pleural opacity (RPO) in a significant proportion of cases. The aim of this study was to investigate which TPE patients would have RPO following the treatment. This study was performed prospectively for a total of 60 TPE patients, who underwent pleural fluid analysis on the initial visit and chest radiographs and computed tomography (CT) scans before and after the administration of antituberculous medication. At the end of antituberculous medication, the incidence of RPO was 68.3% (41/60) on CT with a range of 2-50 mm. Compared with the non-RPO group, the RPO group had a longer symptom duration and lower pleural fluid glucose level. On initial CT, loculation, extrapleural fat proliferation, increased attenuation of extrapleural fat, and pleura-adjacent atelectasis were more frequent, and parietal pleura was thicker in the RPO group compared with the non-RPO group. By multivariate analysis, extrapleural fat proliferation, loculated effusion, and symptom duration were found to be predictors of RPO in TPE. In conclusion, RPO in TPE may be predicted by the clinico-radiologic parameters related to the chronicity of the effusion, such as symptom duration and extrapleural fat proliferation and loculated effusion on CT.
MeSH Terms
Figure
-
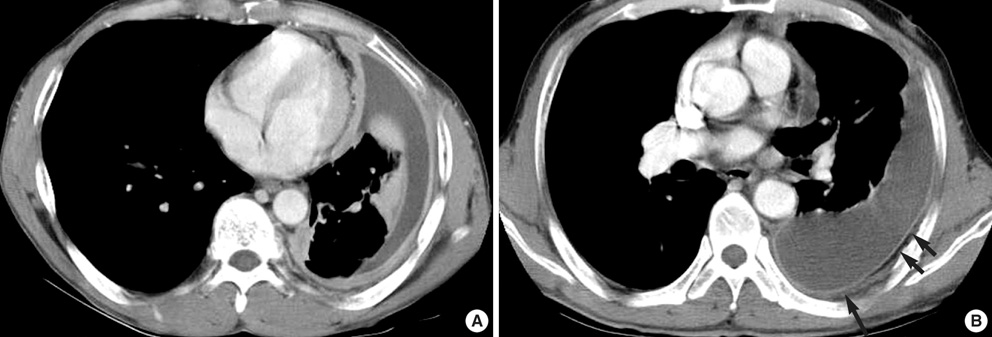
Fig. 1 (A) Initial chest computed tomography (CT) scan shows loculated pleural fluid, accumulated in nondependent portion, and marked circumferential pleural thickening on the left. (B) Enhanced chest CT reveals pleural fluid collection with enhanced, thickened pleura on the left. Extrapleural fat proliferation (> 3 mm, arrows) and increased attenuation of extrapleural fat (a long arrow) are noted.
Reference
-
1. Sahn SA. Pleural thickening, trapped lung, and chronic empyema as sequelae of tuberculous pleural effusion: don't sweat the pleural thickening. Int J Tuberc Lung Dis. 2002. 6:461–464.2. de Pablo A, Villena V, Echave-Sustaeta J, Encuentra AL. Are pleural fluid parameters related to the development of residual pleural thickening in tuberculosis? Chest. 1997. 112:1293–1297.
Article3. Barbas CS, Cukier A, de Varvalho CR, Barbas Filho JV, Light RW. The relationship between pleural fluid findings and the development of pleural thickening in patients with pleural tuberculosis. Chest. 1991. 100:1264–1267.
Article4. Wyser C, Walzl G, Smedema JP, Swart F, van Schalkwyk EM, van de Wal BW. Corticosteroids in the treatment of tuberculous pleurisy. A double-blind, placebo-controlled, randomized study. Chest. 1996. 110:333–338.5. Han DH, Song JW, Chung HS, Lee JH. Resolution of residual pleural disease according to time course in tuberculous pleurisy during and after the termination of antituberculosis medication. Chest. 2005. 128:3240–3245.
Article6. Lee CH, Wang WJ, Lan RS, Tsai YH, Chiang YC. Corticosteroids in the treatment of tuberculous pleurisy. A double-blind, placebo-controlled, randomized study. Chest. 1988. 94:1256–1259.7. Lai YF, Chao TY, Wang YH, Lin AS. Pigtail drainage in the treatment of tuberculous pleural effusions: a randomised study. Thorax. 2003. 58:149–151.
Article8. Kunter E, Ilvan A, Kilic E, Cerrahoglu K, Isitmangil T, Capraz F, Avsart K. The effect of pleural fluid content on the development of pleural thickness. Int J Tuberc Lung Dis. 2002. 6:516–522.
Article9. Yew WW, Leung SK. Prediction of residual pleural thickening in tuberculous pleural effusion. Int J Tuberc Lung Dis. 2003. 7:199–200.10. Giusti G, Galanti B. Bergmeyer HU, editor. Adenosine deaminase. Methods of enzyme analysis. 1983. 3rd ed. New York: Academic Press;315–323.
Article11. Moon JW, Chang YS, Kim SK, Kim YS, Lee HM, Kim SK, Chang J. The clinical utility of polymerase chain reaction for the diagnosis of pleural tuberculosis. Clin Infect Dis. 2005. 41:660–666.
Article12. Wang NS. Anatomy and physiology of the pleural space. Clin Chest Med. 1985. 6:3–16.
Article13. Im JG, Webb WR, Rosen A, Gamsu G. Costal pleura: appearances at high-resolution CT. Radiology. 1989. 171:125–131.
Article14. Waite RJ, Carbonneau RJ, Balikian JP, Umali CB, Pezzella AT, Nash G. Parietal pleural changes in empyema: appearances at CT. Radiology. 1990. 175:145–150.
Article15. Kim HY, Song KS, Lee HJ, Lee JS, Lim TH. Parietal pleura and extrapleural space in chronic tuberculous empyema: CT-pathologic correlation. J Comput Assist Tomogr. 2001. 25:9–15.
Article16. Muller NL. Imaging of the pleura. Radiology. 1993. 186:297–309.
Article17. Uskul B, Turker H, Ulman C, Ertugrul M, Selvi A, Kant A, Arslan S, Ozgel M. The relation of the pleural thickening in tuberculosis pleurisy with the activity of adenosine deaminase. Monaldi Arch Chest Dis. 2005. 63:101–107.
Article18. Candela A, Andujar J, Hernandez L, Martin C, Barroso E, Arriero JM, Romero S. Functional sequelae of tuberculous pleurisy in patients correctly treated. Chest. 2003. 123:1996–2000.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Utility of Pleural Adenosine Deaminase for Diagnosis of Differentiating Tuberculous Pleural Effusion in Children
- Diagnostic Value of Adenosine Deaminase(ADA) and its Isoenzyme in Pleural Effusion
- Factors Associated with Residual Pleural Thickening After Chemotherapy in Tyberculous Pleurisy
- A study on lactic dehydrogenase activity of tuberculous pleural effusion
- Study on Total LDH Activity and LDH Isoenzyme Distribution in Tuberculous and Malignant Pleural Effusions
