Pituitary Carcinoma with Mandibular Metastasis: A Case Report
- Affiliations
-
- 1Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Department of Pathology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. heej0124@ medimail.co.kr
- 3Department of Radiology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- 4Department of Dentistry, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- 5Department of Neurosurgery, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- KMID: 1785804
- DOI: http://doi.org/10.3346/jkms.2007.22.S.S145
Abstract
- Pituitary carcinomas are rare primary adenohypophyseal tumors with cerebrospinal or extracranial metastasis. The present case, the first report of the disease in Korea, involved a 36-yr-old woman who presented with a 3-week history of headache. Brain magnetic resonance imaging revealed a 2.5-cm sellar and suprasellar mass showing heterogeneous enhancement with suspicious invasion of both cavernous sinuses. The patient underwent gross-total resection. The tumor cells were composed of polygonal cells singly or in variable-sized nests. The nuclei were large and round with prominent nucleoli. The cytoplasms was acidophilic and granular. Marked pleomorphism and frequent mitoses (3 per 10 HPFs) were found. By immunohistochemistry, tumor cells were strongly positive for prolactin, but negative for ACTH and GH. Additional immunostainings for cytokeratin, vimentin, and glial fibrillary acidic protein (GFAP) were negative. After the surgery, the patient received radiotherapy because of the atypical histologic features. The prolactin level fell from 123.17 ng/mL to 5.17 ng/mL after surgery. Nine months after the initial diagnosis, the patient died from mandibular metastasis associated with the pituitary carcinoma.
Keyword
MeSH Terms
Figure
-
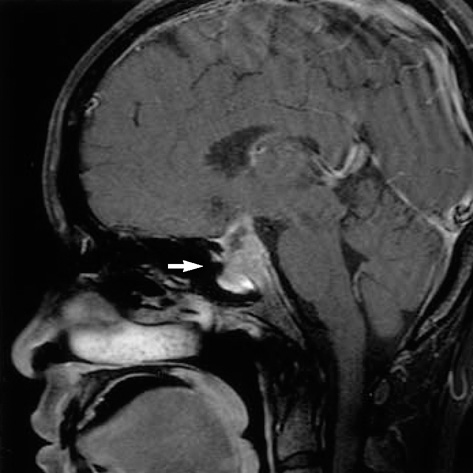
Fig. 1 Sagittal contrast enhanced T1-weighted image showing a lobulating contoured mass (arrow) with heterogeneous enhancement in the sella. Invasion of the posterior wall of the sphenoid sinus by the sella mass is evident.

Fig. 2 Resected tumor cells showing variable-sized nests and single cells (left lower) mixed with adenohypophyseal cells of normal appearance (right upper) (H&E stain, ×100).

Fig. 3 Tumor cells showing atypical morphology with large round nuclei and prominent nucleoli. The mitoses are 3/10 high power fields (H&E, ×400).

Fig. 4 Tumor cells showing strong and diffuse positive staining for prolactin (Prolactin, ×400).

Fig. 5 (A) Positive immunostaining for p53 in the primary pituitary tumor (×400). (B) High (10%) Ki-67 labeling index (×400).
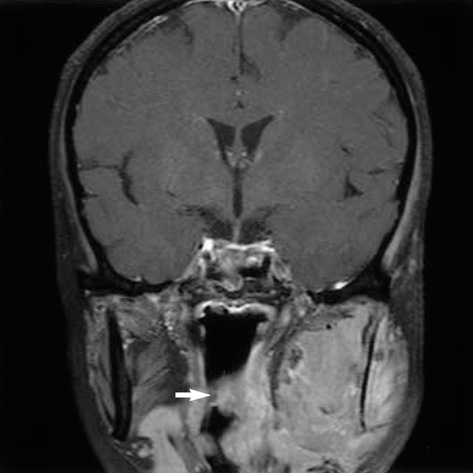
Fig. 6 Follow-up coronal contrast enhanced T1-weighted image showing an ill-defined heterogeneously-enhanced soft tissue mass (arrow) with destruction of the left mandible. Left oropharyngeal wall-thickening, suggesting spread of the tumor, is also evident.

Fig. 7 Histopathologic and immunologic features of the metastatic tumor showing similarity to that of the primary pituitary tumor (H&E stain, ×400).
Reference
-
1. Pernicone PJ, Scheithauer BW, Sebo TJ, Kovacs KT, Horvath E, Young WF Jr, Lloyd RV, Davis DH, Guthrie BL, Schoene WC. Pituitary carcinoma: a clinicopathologic study of 15 cases. Cancer. 1997. 79:804–812.2. Cairns H, Russel DS. Intracranial and spinal metastasis in gliomas of the brain. Brain. 1931. 54:377–420.3. Scheithauer BW, Kovacs KT, Horvath E, Roncaroli F, Ezzat S, Asa SL, Lloid RV, Nose V, Watwon RE Jr, Lindell EP. DeLellis RA, Lloyd RV, Hritz PU, Eng C, editors. Pituitary carcinoma. Pathology & Genetics Tumours of Endocrine Organs. 2004. Lyon, France: International Agency for Research on Cancer (IARC) Press;36–39.4. Long MA, Colquhoun IR. Case report: multiple intra-cranial metastases from a prolactin-secreting pituitary tumour. Clin Radiol. 1994. 49:356–358.
Article5. Bayindir C, Balak N, Gazioglu N. Prolactin-secreting carcinoma of the pituitary: clinicopathological and immunohistochemical study of a case with intracranial and intraspinal dissemination. Br J Neurosurg. 1997. 11:350–355.6. Lamas C, Nunez R, Garcia-Uria J, Salas C, Saucedo G, Estrada J, Parajon A, Lucas T. Malignant prolactinoma with multiple bone and pulmonary metastases. Case report. J Neurosurg. 2004. 101:Suppl 1. 116–121.7. Thapar K, Kovacs K, Scheithauer BW, Stefaneanu L, Horvath E, Pernicone PJ, Murray D, Laws ER Jr. Proliferative activity and invasiveness among pituitary adenomas and carcinomas: an analysis using the MIB-1 antibody. Neurosurgery. 1996. 38:99–106.
Article8. Yamashita H, Nakagawa K, Tago M, Nakamura N, Shiraishi K, Yamauchi N, Ohtomo K. Pathological changes after radiotherapy for primary pituitary carcinoma: a case report. J Neurooncol. 2005. 75:209–214.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Metastasis of Hepatocellular Carcinoma to Pituitary Adenoma: A Case Report
- Drop Metastasis of Adrenocorticotropic Hormone-Producing Pituitary Carcinoma to the Cauda Equina
- Ovarian and Pituitary Metastasis from Adenocarcinoma of the Lung: A Case Report
- Differential Diagnosis and Management of a Pituitary Mass with Renal Cell Carcinoma
- Metastatic hepatocellular carcinoma on the mandible: A case report
