Balloon Dilatation for Corrosive Esophageal Strictures in Children: Radiologic and Clinical Outcomes
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine and the Institute of Radiation Medicine, SNUMRC, Seoul 110-744, Korea. kimws@radcom.snu.ac.kr
- KMID: 1783197
- DOI: http://doi.org/10.3348/kjr.2010.11.2.203
Abstract
OBJECTIVE
We retrospectively evaluated the effectiveness of the esophageal balloon dilatation (EBD) in children with a corrosive esophageal stricture.
MATERIALS AND METHODS
The study subjects included 14 patients (M:F = 8:6, age range: 17-85 months) who underwent an EBD due to a corrosive esophageal stricture. The causative agents for the condition were glacial acetic acid (n = 9) and lye (n = 5).
RESULTS
A total of 52 EBD sessions were performed in 14 patients (range 1-8 sessions). During the mean 15-month follow-up period (range 1-79 months), 12 patients (86%) underwent additional EBD due to recurrent esophageal stricture. Dysphagia improved after each EBD session and oral feeding was possible between EBD sessions. Long-term success (defined as dysphagia relief for at least 12 months after the last EBD) was achieved in two patients (14%). Temporary success of EBD (defined as dysphagia relief for at least one month after the EBD session) was achieved in 17 out of 52 sessions (33%). A submucosal tear of the esophagus was observed in two (4%) sessions of EBD.
CONCLUSION
Only a limited number of children with corrosive esophageal strictures were considered cured by EBD. However, the outcome of repeated EBD was sufficient to allow the children to eat per os prior to surgical management.
Keyword
MeSH Terms
-
Acetic Acid/poisoning
Balloon Dilatation/*methods
Burns, Chemical/radiography/*therapy
Caustics/poisoning
Child
Child, Preschool
Deglutition Disorders/etiology
Esophageal Stenosis/chemically induced/*radiography/*therapy
Esophagus/radiography
Female
Humans
Infant
Lye/poisoning
Male
Retrospective Studies
Treatment Outcome
Figure
-
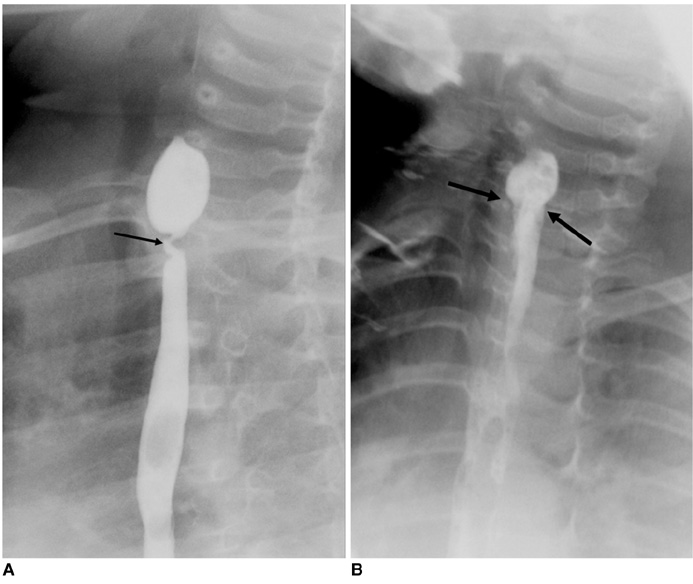
Fig. 1 2-year-old boy with focal esophageal stricture after glacial acetic acid ingestion (patient 9) A. Initial esophagogram obtained four months after ingestion revealed severe focal stricture (arrow) in upper esophagus. B. Esophagogram obtained after esophageal balloon dilatation using 10 mm balloon catheter demonstrated improvement of stricture (arrows). Patient's feeding difficulty was substantially relieved. However, recurrent stenosis occurred after four sessions of esophageal balloon dilatation, which led to performing segmental resection and anastomosis.
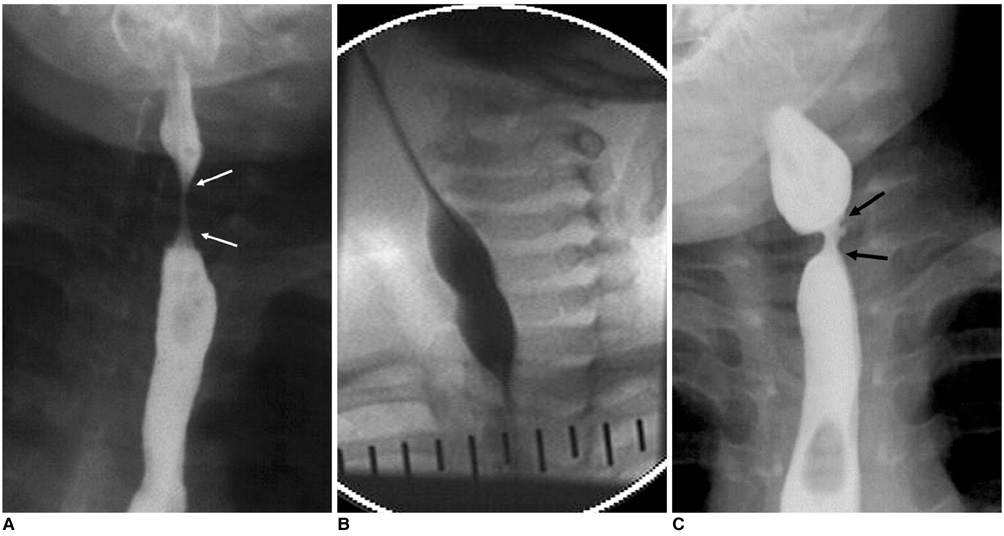
Fig. 2 1-year-old girl with segmental stricture after ingesting glacial acetic acid (patient 14). A. Initial esophagogram obtained one month after ingestion of glacial acetic acid revealed segmental stricture (arrows) in upper esophagus. B. Initial esophageal balloon dilatation was performed with 8 mm balloon catheter. 'Hourglass' deformity of balloon at level of stricture was eliminated (not shown here) when inflation was maintained. C. Esophagogram obtained one month after second esophageal balloon dilatation session shows stricture recurrence (arrows). After four esophageal balloon dilatation sessions, segmental resection and anastomosis was performed.
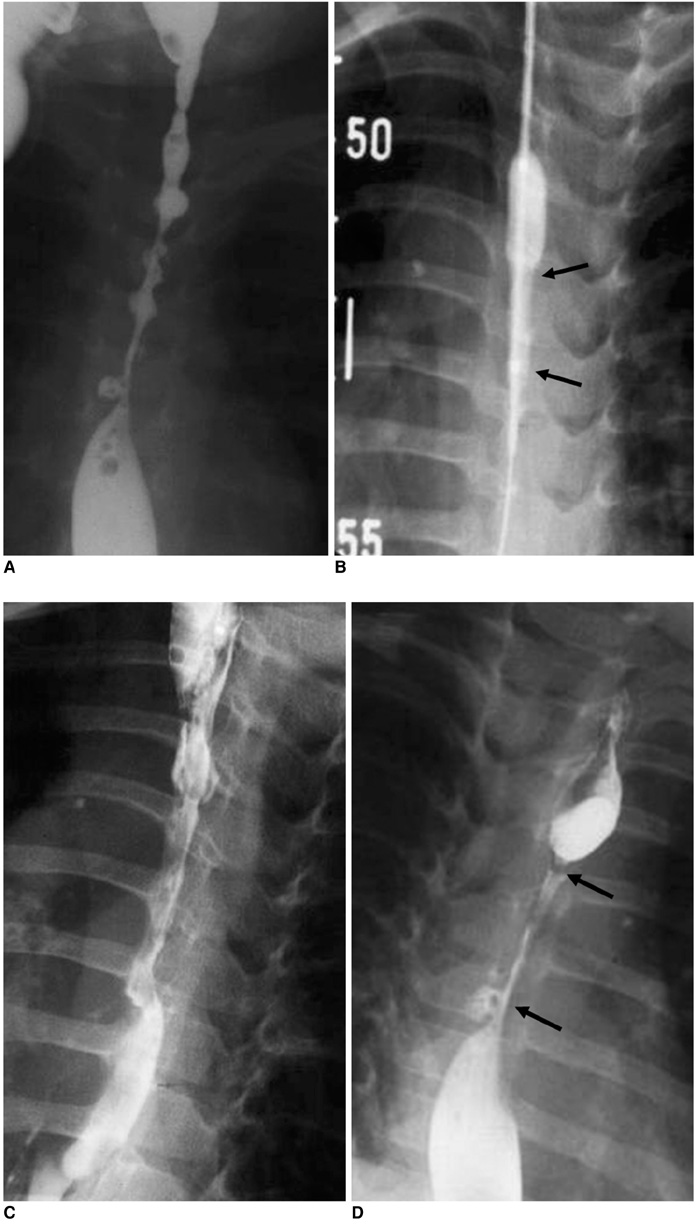
Fig. 3 2-year-old girl with diffuse stricture after lye ingestion (patient 2). A. Initial esophagogram obtained six months after lye ingestion reveals diffuse irregular stricture of esophagus. B. Esophageal balloon dilatation was performed with 8 mm balloon catheter. Note incomplete balloon dilatation (arrows) due to presence of severe fibrotic changes. C. Esophagogram obtained after above esophageal balloon dilatation session demonstrates some improvement. D. Follow-up esophagogram obtained two weeks after esophageal balloon dilatation demonstrates diffuse restricture (arrows) in esophagus.
Reference
-
1. Huang YC, Ni YH, Lai HS, Chang MH. Corrosive esophagitis in children. Pediatr Surg Int. 2004. 20:207–210.2. Song HY, Han YM, Kim HN, Kim CS, Choi KC. Corrosive esophageal stricture: safety and effectiveness of balloon dilation. Radiology. 1992. 184:373–378.3. Park JY, Shin JY, Yang HR, Ko JS, Kim WS, Seo JK. Usefulness of early endoscopy for predicting the development of stricture after corrosive esophagitis in children. Korean J Pediatr. 2009. 52:446–452.4. Hamza AF, Abdelhay S, Sherif H, Hasan T, Soliman H, Kabesh A, et al. Caustic esophageal strictures in children: 30 years' experience. J Pediatr Surg. 2003. 38:828–833.5. Weintraub JL, Eubig J. Balloon catheter dilatation of benign esophageal strictures in children. J Vasc Interv Radiol. 2006. 17:831–835.6. London RL, Trotman BW, DiMarino AJ Jr, Oleaga JA, Freiman DB, Ring EJ, et al. Dilatation of severe esophageal strictures by an inflatable balloon catheter. Gastroenterology. 1981. 80:173–175.7. Goldthorn JF, Ball WS Jr, Wilkinson LG, Seigel RS, Kosloske AM. Esophageal strictures in children: treatment by serial balloon catheter dilatation. Radiology. 1984. 153:655–658.8. Sato Y, Frey EE, Smith WL, Pringle KC, Soper RT, Franken EA Jr. Balloon dilatation of esophageal stenosis in children. AJR Am J Roentgenol. 1988. 150:639–642.9. Ko HK, Shin JH, Song HY, Kim YJ, Ko GY, Yoon HK, et al. Balloon dilation of anastomotic strictures secondary to surgical repair of esophageal atresia in a pediatric population: long-term results. J Vasc Interv Radiol. 2006. 17:1327–1333.10. Lisy J, Hetkova M, Snajdauf J, Vyhnanek M, Tuma S. Long-term outcomes of balloon dilation of esophageal strictures in children. Acad Radiol. 1998. 5:832–835.11. Fasulakis S, Andronikou S. Balloon dilatation in children for oesophageal strictures other than those due to primary repair of oesophageal atresia, interposition or restrictive fundoplication. Pediatr Radiol. 2003. 33:682–687.12. Lan LC, Wong KK, Lin SC, Sprigg A, Clarke S, Johnson PR, et al. Endoscopic balloon dilatation of esophageal strictures in infants and children: 17 years' experience and a literature review. J Pediatr Surg. 2003. 38:1712–1715.13. Doo EY, Shin JH, Kim JH, Song HY. Oesophageal strictures caused by the ingestion of corrosive agents: effectiveness of balloon dilatation in children. Clin Radiol. 2009. 64:265–271.14. Kukkady A, Pease PW. Long-term dilatation of caustic strictures of the oesophagus. Pediatr Surg Int. 2002. 18:486–490.15. Yeming W, Somme S, Chenren S, Huiming J, Ming Z, Liu DC. Balloon catheter dilatation in children with congenital and acquired esophageal anomalies. J Pediatr Surg. 2002. 37:398–402.16. Yararbai O, Osmanodlu H, Kaplan H, Tokat Y, Coker A, Korkut M, et al. Esophagocoloplasty in the management of postcorrosive strictures of the esophagus. Hepatogastroenterology. 1998. 45:59–64.17. Ragheb MI, Ramadan AA, Khalia MA. Management of corrosive esophagitis. Surgery. 1976. 79:494–498.18. Kim JH, Song HY, Kim HC, Shin JH, Kim KR, Park SW, et al. Corrosive esophageal strictures: long-term effectiveness of balloon dilatation in 117 patients. J Vasc Interv Radiol. 2008. 19:736–741.19. Lovejoy FH Jr. Corrosive injury of the esophagus in children: failure of corticosteroid treatment reemphasizes prevention. N Engl J Med. 1990. 323:668–670.20. Muhletaler CA, Gerlock AJ Jr, de Soto L, Halter SA. Acid corrosive esophagitis: radiographic findings. AJR Am J Roentgenol. 1980. 134:1137–1140.21. de Lange EE, Shaffer HA Jr. Anastomotic strictures of the upper gastrointestinal tract: results of balloon dilation. Radiology. 1988. 167:45–50.22. McLean GK, Cooper GS, Hartz WH, Burke DR, Meranze SG. Radiologically guided balloon dilation of gastrointestinal strictures. Part I. Technique and factors influencing procedural success. Radiology. 1987. 165:35–40.23. Kim IO, Yeon KM, Kim WS, Park KW, Kim JH, Han MC. Perforation complicating balloon dilation of esophageal strictures in infants and children. Radiology. 1993. 189:741–744.24. Maynar M, Guerra C, Reyes R, Mayor J, Garcia J, Facal P, et al. Esophageal strictures: balloon dilation. Radiology. 1988. 167:703–706.25. Jayakrishnan VK, Wilkinson AG. Treatment of oesophageal strictures in children: a comparison of fluoroscopically guided balloon dilatation with surgical bouginage. Pediatr Radiol. 2001. 31:98–101.26. Han HY, Song HY, Han YM, Chon SB, Chung GH, Sohn MH, et al. Difficulty of balloon dilatation in corrosive esophageal strictures. J Korean Radiol Soc. 1993. 29:1181–1186. [Korean].27. Gundogdu HZ, Tanyel FC, Buyukpamukcu N, Hicsonmez A. Conservative treatment of caustic esophageal strictures in children. J Pediatr Surg. 1992. 17:767–770.28. Wilkinson AG, MacKinlay GA. Use of a cutting balloon in the dilatation of caustic oesophageal stricture. Pediatr Radiol. 2004. 34:414–416.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Difficulty of balloon dilatation in corrosive esophageal strictures
- Balloon catheter dilatation of esophageal strictures
- Balloon catheter dilatation of esophageal strictures in children and an infant
- The Effect of Bougie and Balloon Dilatation on Benign Esophageal Stricture
- A Single Center Experience of Self-Bougienage on Stricture Recurrence after Surgery for Corrosive Esophageal Strictures in Children
