CT and MR Imaging of the Buccal Space: Normal Anatomy and Abnormalities
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Institute of Radiation Medicine, SNUMRC, and Clinical Research Institute, Seoul National University Hospital, Korea. hanmh@radcom.snu.ac.kr
- KMID: 1783169
- DOI: http://doi.org/10.3348/kjr.2005.6.1.22
Abstract
- The buccal space is an anatomical compartment lying anterior to the masticator space and lateral to the buccinator muscle. Since the major purpose of imaging is to define the likely anatomic origin and also the extent of a given lesion, thorough knowledge of the normal anatomy of the buccal space is essential, and this knowledge can aid the physician in narrowing down the list of possible maladies on the differential diagnosis. We illustrate here in this paper the important anatomic landmarks and typical pathologic conditions of the buccal space such as the developmental lesions and the neoplastic lesions. Knowledge of the expected pathologic conditions is useful for the radiologist when interpreting facial CT and MR images.
Keyword
MeSH Terms
Figure
-
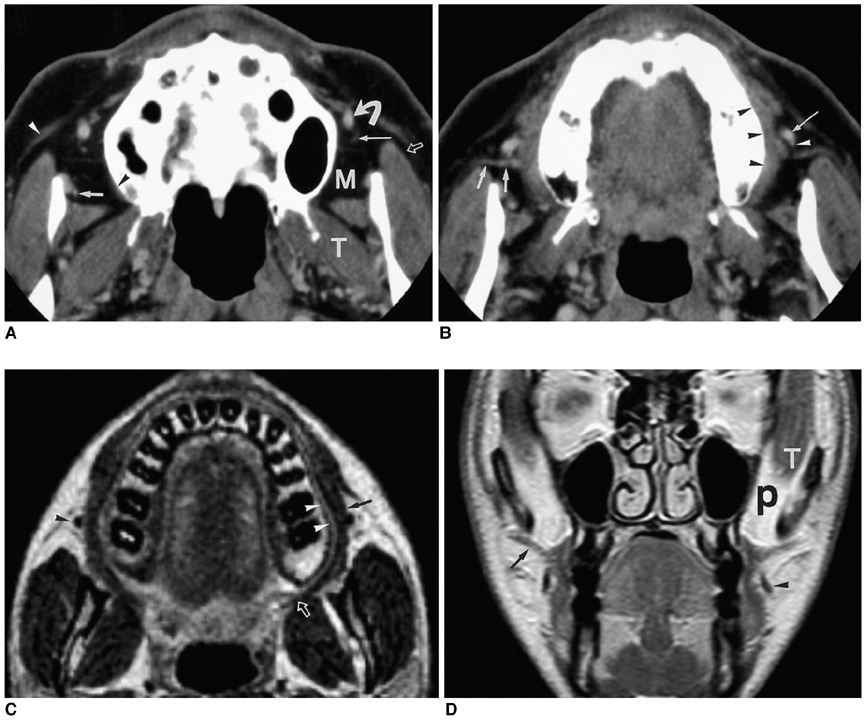
Fig. 1 The normal anatomy of the buccal space. A. A transverse enhanced CT scan at the level of the upper buccal space shows the lateral projection (open arrow) of buccal fat lateral to the masseter muscle and the medial projection (M) of buccal fat between the masseter muscle and the maxilla. The posterior extent of the medial buccal fat pad is limited by the lateral pterygoid muscle (T) and the overlying fascia. The origin of the buccinator muscle is seen on the right side (black arrowhead). The facial vein (curved arrow) is seen located within the buccal space. The facial artery (long arrow), buccal artery (short arrow), and zygomaticus muscle (white arrowhead) are noted. B. A transverse enhanced CT scan at the level of the middle buccal space shows the parotid duct (short arrows) coursing through the buccal space. The angular portion of the facial vein (arrow) and facial artery (arrowhead) are located anterior to the duct. The buccinator muscle (black arrowheads) is also noted. C. A transverse T2-weighted MR image at the level of the lower buccal space shows the buccinator muscle (arrow) having a low signal intensity and the submucosal fat pad (arrowheads) having a high signal intensity. The insertion of the buccinator muscle on the pterygomandibular raphe (open arrow) is also visible at this level. The facial vein (arrowhead) appears as a signal void. D. A coronal enhanced T1-weighted MR image shows the parotid duct (arrow), facial vein (arrowhead), and buccinator muscle. The deep portion of the buccal fat pad (P) lies between the temporal muscle (T) and the maxillary sinus.

Fig. 2 Bilateral accessory parotid tissues in a 59-year-old man. A transverse enhanced CT scan shows the bilateral accessory parotid tissues (arrows), which have the same attenuation as the tissue in the main parotid gland.
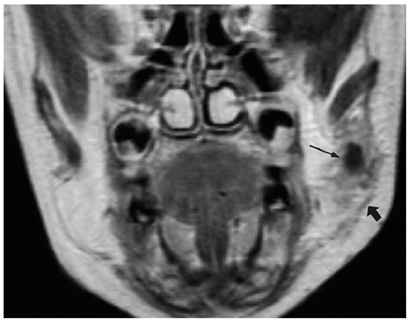
Fig. 3 Infected dermoid cyst in a 3-year-old girl. A coronal enhanced T1-weighted MR image shows the cystic mass (thin arrow) in the left buccal space. The mass has an irregular margin and it has infiltrated into the surrounding buccal fat pad. Note the thickening of the superficial muscles of facial expression and the investing fascia (thick arrow).
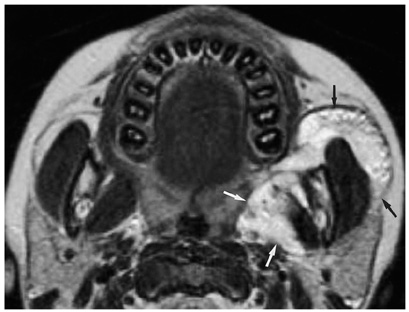
Fig. 4 Hemangioma in a 5-year-old girl. A transverse T2-weighted MR image shows an irregular mass (arrows) having high signal intensity involving the buccal space and the masticator space.
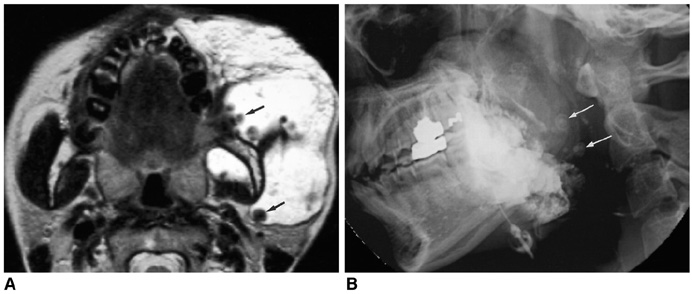
Fig. 5 Venous malformation in a 22-year-old woman. A. A transverse T2-weighted MR image shows a high signal intensity mass lesion occupying the buccal space and the masticator space. Note the multiple phleboliths (arrows) having low signal intensity. B. The lateral radiograph obtained after the percutaneous injection of an ethanolamine oleate and iodized oil mixture shows the radiopaque cast filling the vascular space of the lesion. Note the multiple laminated phleboliths (arrows).
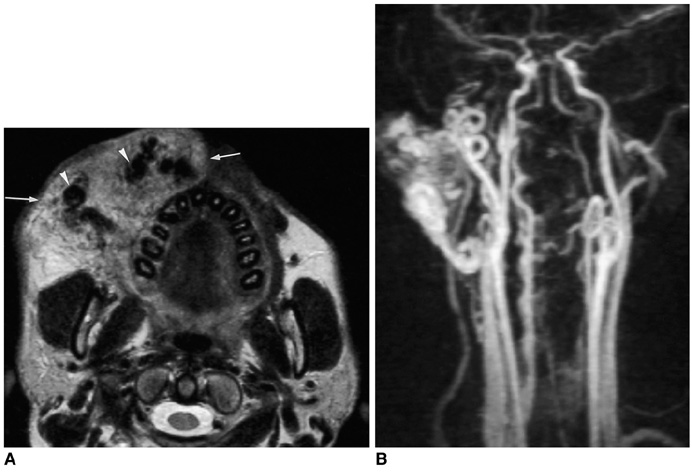
Fig. 6 Arteriovenous malformation in a 32-year-old man. A. A transverse T2-weighted MR image shows the intermediate signal intensity mass lesion (arrows) with multiple signal voids (arrowheads) in the right buccal space. B. A MR angiography shows the tortuous and dilated facial artery and the internal maxillary artery.

Fig. 7 Cystic lymphangioma in a 2-year-old boy. A transverse T2-weighted MR image shows multiple cystic lesions with fluid-fluid levels (arrowheads).
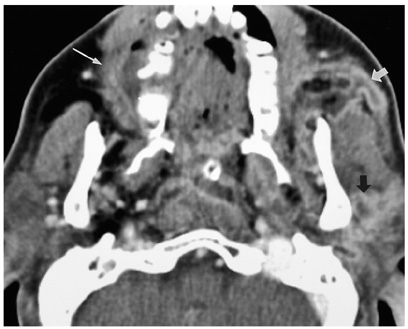
Fig. 8 Abscess in a 60-year-old man. A transverse enhanced CT scan shows a multiloculated low-density area (thick arrows) with peripheral rim enhancement in the left buccal space, parotid space and parapharyngeal space. Note the right periapical abscesses confined by the right buccinator (thin arrow).
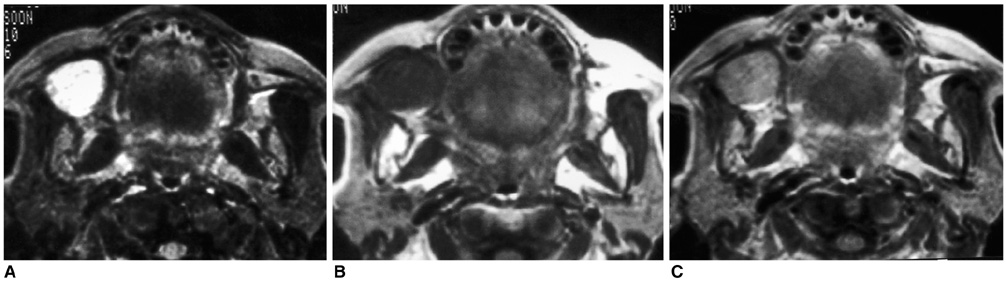
Fig. 9 Pleomorphic adenoma in a 65-year-old woman. A. A transverse T2-weighted MR image shows a round, well-defined mass with bright signal intensity in the right buccal space. B. A transverse T1-weighted MR image shows a round mass with low signal intensity in the right buccal space. C. An enhanced transverse T1-weighted MR image shows homogeneous enhancement of the lesion.

Fig. 10 Adenoid cystic carcinoma in a 75-year-old woman. A. A transverse T2-weighted MR image shows a small round mass (arrows) with central bright signal intensity. Note the ill-defined infiltration of high signal intensity into the right buccinator muscle (arrowheads). B. An enhanced transverse T1-weighted MR image shows peripheral enhancement (arrows) of the mass. Note the ill-defined infiltration into the right buccinator muscle (arrowheads) with good enhancement.
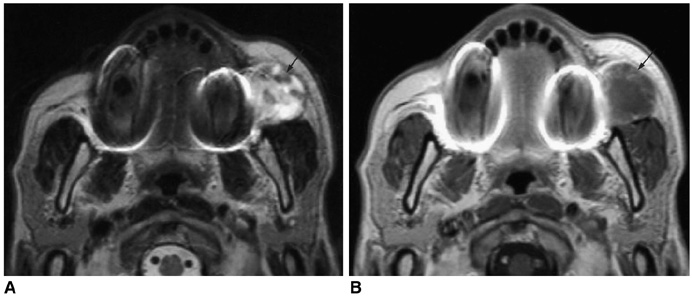
Fig. 11 Carcinoma ex pleomorphic adenoma in a 70-year-old man. A. A transverse T2-weighted MR image shows a round mass of bright signal intensity and small, low signal intensity spots in the left buccal space (arrow). B. An enhanced transverse T1-weighted MR image shows the mildly enhancing foci (arrow).

Fig. 12 Rhabdomyosarcoma in a 15-year-old girl. A. A transverse T2-weighted MR image shows a round, well-demarcated mass of high signal intensity in the right buccal space. B. An enhanced coronal T1-weighted MR image shows the heterogeneous enhancement of the lesion.
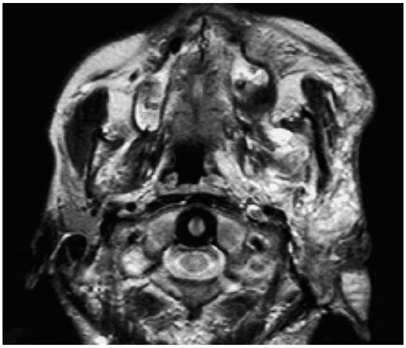
Fig. 13 Plexiform neurofibroma in a 20-year-old man. A transverse T2-weighted MR image shows ill-defined high signal intensity mass involving the buccal space, masticator space, parapharyngeal space, parotid space and auricle.
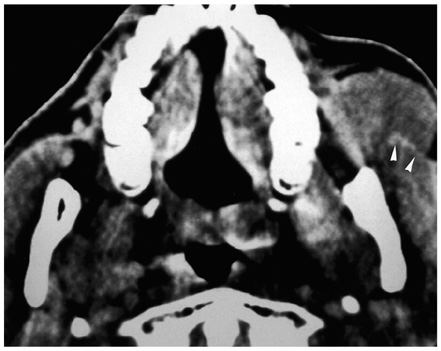
Fig. 14 Non-Hodgkin lymphoma of the diffuse small cell type in a 49-year-old man. A transverse CT scan shows a homogeneous solid mass in the left buccal space. Note the molding pattern of the mass and the lack of mass effect on the left masseter muscle (arrowheads).

Fig. 15 Peripheral T-cell lymphoma in a 57-year-old woman. A. A transverse CT scan shows the ill-defined infiltrative lesions in both the buccal space and the subcutaneous layer on the right cheek. Note the overlying skin thickening (arrowhead). B. A transverse T1-weighted MR image shows the ill-defined infiltrative lesions in the same area.

Fig. 16 Surgically confirmed metastatic lymphadenopathy in a 71-year-old man. A transverse T2-weighted MR image shows a well-circumscribed mass (arrow) with central high signal intensity. The patient underwent left partial mandibulectomy due to squamous cell carcinoma of the gingiva.
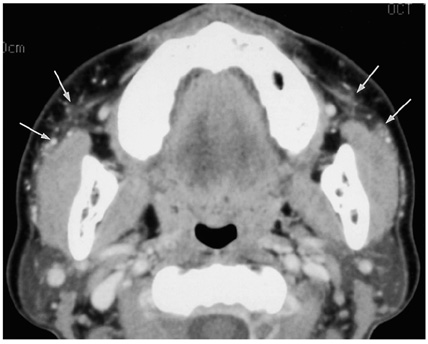
Fig. 17 Foreign body granuloma in a 49-year-old woman with a history of paraffin injection into both cheeks 20 years ago. A transverse enhanced CT scan shows the ill-defined infiltration (arrows) and several small calcifications around the bilateral buccal spaces.

Fig. 18 Kimura disease in a 14-year-old boy. A. A transverse T2-weighted MR image shows an infiltrative mass-like lesion (arrow) having high signal intensity in the left buccal space. B. A transverse enhanced T1-weighted MR image shows moderate enhancement of the lesion.
Reference
-
1. Tart RP, Kotzur IM, Mancuso AA, Glantz MS, Mukherji SK. CT and MR imaging of the buccal space and buccal space masses. RadioGraphics. 1995. 15:531–550.2. Smoker WRK. Som PM, Curtin HD, editors. Oral cavity. Head and neck imaging. 1996. 3rd ed. St. Louis: Mosby;488–544.3. Kurabayashi T, Ida M, Tetsumura A, Ohbayashi N, Yasumoto M, Sasaki T. MR imaging of benign and malignant lesions in the buccal space. Dentomaxillofac Radiol. 2002. 31:344–349.4. Kurabayashi T, Ida M, Yoshino N, Sasaki T, Kishi T, Kusama M. Computed tomography in the diagnosis of buccal space masses. Dentomaxillofac Radiol. 1997. 26:347–353.5. Werner JA, Dunne AA, Folz BJ, Rochels R, Bien S, Ramaswamy A, et al. Current concepts in the classification, diagnosis and treatment of hemangiomas and vascular malformations of the head and neck. Eur Arch Otorhinolaryngol. 2001. 258:141–149.6. Baker LL, Dillon WP, Hieshima GB, Dowd CF, Frieden IJ. Hemangiomas and vascular malformations of the head and neck: MR characterization. AJNR Am J Neuroradiol. 1993. 14:307–314.7. Kern S, Niemeyer C, Darge K, Merz C, Laubenberger J, Uhl M. Differentiation of vascular birthmarks by MR imaging. An investigation of hemangiomas, venous and lymphatic malformations. Acta Radiol. 2000. 41:453–457.8. Sigal R, Monnet O, de Baere T, Micheau C, Shapeero LG, Julieron M, et al. Adenoid cystic carcinoma of the head and neck: evaluation with MR imaging and clinical-pathologic correlation in 27 patients. Radiology. 1992. 184:95–101.9. Shah GV. MR imaging of salivary glands. Magn Reson Imaging Clin N Am. 2002. 10:631–662.10. Kim HC, Han MH, Kim KH, Jae HJ, Lee SH, Kim SS, et al. Primary thyroid lymphoma: CT findings. Eur J Radiol. 2003. 46:233–239.11. Lee HJ, Im JG, Goo JM, Kim KW, Choi BI, Chang KH, et al. Peripheral T-cell lymphoma: spectrum of imaging findings with clinical and pathologic features. RadioGraphics. 2003. 23:7–26.12. Moon WK, Park JM, Kim YI, et al. Inflammatory and infectious Diseases of the breast: Imaging Findings. Postgraduate Radiol. 2000. 20:131–141.13. Som PM, Biller HF. Kimura disease involving parotid gland and cervical nodes: CT and MR findings. J Comput Assist Tomogr. 1992. 16:320–322.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of Normal Anatomy of Oral Cavity in Open-mouth View with CT and MRI: Comparison with Closed-mouth View
- Buccal Space Lesions: A New Classification Based on CT and MR Imaging Findings
- Spontaneous rupture of intrasellar cyst demonstrated by CT and MR imaging
- Inflammatory Pseudotumor of the Extraorbital Head and Neck: CT and MR Imaging Findings
- Detection of Acute Intraventricular Hemorrhage: Comparison of FLAIR MR Imaging with Unenhanced CT
