Brucella Endocarditis with Splenic Abscess: A Report of the First Case Diagnosed in Korea
- Affiliations
-
- 1Department of Internal Medicine, Eulji University College of Medicine, Daejeon, Korea. yhj822@medimail.co.kr
- 2Division of Zoonoses, Center for Immunology and Pathology, National Institutes of Health, Seoul, Korea.
- KMID: 1782980
- DOI: http://doi.org/10.3349/ymj.2009.50.1.142
Abstract
- Human brucellosis has a broad spectrum of clinical manifestations, which includes endocarditis, a focal complication that is uncommon yet responsible for the majority of associated deaths. The most successful treatment outcomes of Brucella endocarditis have been reported with usage of both antimicrobial agents and surgery. However, there are few reports on the treatment of Brucella endocarditis using antibiotics only. We report the first case in Korea of Brucella endocarditis with aortic valve vegetations and an accompanying splenic abscess, which were treated successfully with antibiotic therapy alone.
Keyword
MeSH Terms
Figure
-
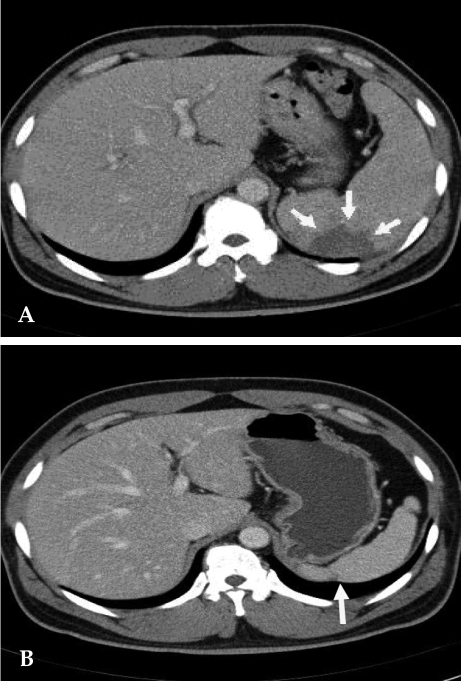
Fig. 1 (A) Contrast-enhanced abdomen CT scan reveals partial splenic abscess that is a wedge shape (arrow) and splenomegaly. (B) Twelve months later, follow-up CT scan reveals normalized spleen size of about 11 cm compared with the previous splenomegaly size of 15 cm. A portion of the splenic abscess changed into cortical dimpling (arrow) with segmental shrinkage.
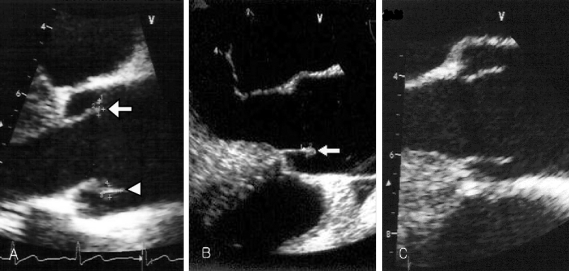
Fig. 2 (A) Transesophageal echocardiography reveals one vegetation (4 × 2 mm, arrow) on the right aortic coronary cusp and the other vegetation (5 × 3 mm, arrow head) on the noncoronary aortic cusp upon admission. (B) Two months later, follow up transesophageal echocardiography (TEE) reveals no interval change of the vegetation (arrow) size within the noncoronary cusp, but vegetation within the right coronary cusp was completely resolved. (C) Seven months later, follow up TEE shows complete resolution of the remained vegetation.

Fig. 3 Genus-specific PCR. Molecular diagnostic assays based on PCR amplification of different genomic targets for the identification of Brucella spp. tested of the isolate. The clinical isolate was tested by the conventional biochemical tests and detected with common genes (BCSP-31 kDa, OMP2-36kDa, 16S rRNA) of Brucella spp. M, 100 bp marker; Lane 1, Brucella abortus ATCC 2308; Lane 2, Patient's isolate.
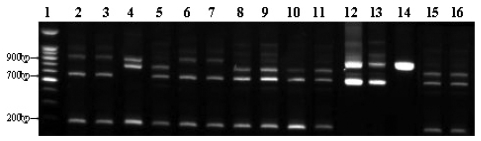
Fig. 4 Species-specific AMOS-Multi-PCR. We have adopted Multiplex AMOS-PCR method for the species-specific typing of clinical isolate. In the profile of Multiplex AMOS-PCR, B. abortus (biovar 1, 2, 3, 4, 6), B. melitensis (biovar 1, 2), B. canis, and B. suis (biovar 3) showed characterization patterns into the respective species and four different amplification patterns were observed. Multiplex AMOS-PCR patterns I (200, 600 and 900 bp) were B. melitensis (biovar 1, 2), B. abortus (biovar 3, 6), patterns II (200, 600 and 720 bp) were B. abortus (biovar 1, 2, 4), patterns III (600 and 900 bp) were B. canis, B. suis (biovar 3) and patterns IV (200, 720 and 900 bp) were B. abortus ATCC 7705. The clinical isolate of our patient had identical patterns as B. abortus biovar 1 (patterns II). Lane 1, 100 bp ladder; Lane 2 & 3, B. melitensis; Lane 4, B. abortus ATCC 7705; Lane 5, B. abortus bv.1; Lane 6, B. abortus bv. 3; Lane 7, B. abortus bv.6; Lane 8, B. abortus bv.2; Lane 9, B. abortus bv4; Lane 10, S19; Lane 11, RB51; Lane 12, B. canis; Lane 13, B. suis; Lane 14, B. ovis; Lane 15, other patient's isolate (B. abortus bv.1); Lane 16, our patient's isolate.
Cited by 1 articles
-
Splenic Infarction Associated with Brucellosis in a Non-Endemic Area
Jae Hoon Lee, Yu Min Lee, Chang Hoon Lee, Chang Soo Choi, Tae Hyeon Kim
Infect Chemother. 2010;42(1):48-50. doi: 10.3947/ic.2010.42.1.48.
Reference
-
1. Young EJ. Mandell GL, Bennett JE, Dolin R, editors. Brucella species. Principles and practice of infectious diseases. 2000. 5th ed. New York: Churchill Livingstone;p. 2386–2391.2. Mert A, Kocak F, Ozaras R, Tabak F, Bilir M, Kucukuglu S, et al. The role of antibiotic treatment alone for the management of Brucella endocarditis in adults: a case report and literature review. Ann Thorac Cardiovasc Surg. 2002; 8:381–385. PMID: 12517300.3. Memish Z, Mah MW, Al Mahmoud S, Al Shaalan M, Khan MY. Brucella bacteraemia: clinical and laboratory observations in 160 patients. J Infect. 2000; 40:59–63. PMID: 10762113.4. Park MS, Woo YS, Lee MJ, Shim SK, Lee HK, Choi YS, et al. The first case of human brucellosis in Korea. Infect Chemother. 2003; 35:461–466.5. Peery TM, Belter LF. Brucellosis and heart disease. II. Fatal brucellosis: a review of the literature and report of new cases. Am J Pathol. 1960; 36:673–697. PMID: 14431371.6. KCDC. Korea Center for Disease Control and Prevention. CDWR. 2006; 52:1–36.7. Young EJ. Mandell GL, Bennett JE, Dolin R, editors. Brucella species. Principles and practice of infectious diseases. 1995. 4th ed. New York: Churchill Livingstone;p. 2053–2060.8. Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Duke Endocarditis Service. Am J Med. 1994; 96:200–209. PMID: 8154507.9. Delvecchio G, Fracassetti O, Lorenzi N. Brucella endocarditis. Int J Cardiol. 1991; 33:328–329. PMID: 1743797.10. al-Mudallal DS, Mousa AR, Amin Marafie AA. Apyrexic Brucella melitensis aortic valve endocarditis. Trop Geogr Med. 1989; 41:372–376. PMID: 2635455.11. Caldarera I, Albanese S, Piovaccari G, Ferlito M, Galli R, Squadrini F, et al. Brucella endocarditis: role of drug treatment associated with surgery. Cardiologia. 1996; 41:465–467. PMID: 8767636.12. Kumar N, Prabhakar G, Kandeel M, Mohsen IZ, Awad M, al-Halees Z, et al. Brucella mycotic aneurysm of ascending aorta complicating discrete subaortic stenosis. Am Heart J. 1993; 125:1780–1782. PMID: 8498327.13. al-Harthi SS. The morbidity and mortality pattern of brucella endocarditis. Int J Cardiol. 1989; 25:321–324. PMID: 2613379.
Article14. Fernández-Guerrero ML. Zoonotic endocarditis. Infect Dis Clin North Am. 1993; 7:135–152. PMID: 8463649.15. Young EJ. An overview of human brucellosis. Clin Infect Dis. 1995; 21:283–289. quiz 290. PMID: 8562733.
Article16. Bayer AS, Bolger AF, Taubert KA, Wilson W, Steckelberg J, Karchmer AW, et al. Diagnosis and management of infective endocarditis and its complications. Circulation. 1998; 98:2936–2948. PMID: 9860802.
Article17. Arslan H, Korkmaz ME, Kart H, Gül C. Management of brucella endocarditis of a prosthetic valve. J Infect. 1998; 37:70–71. PMID: 9733385.
Article18. Reguera JM, Alarcón A, Miralles F, Pachón J, Juárez C, Colmenero JD. Brucella endocarditis: clinical, diagnostic, and therapeutic approach. Eur J Clin Microbiol Infect Dis. 2003; 22:647–650. PMID: 14566576.19. Flugelman MY, Galun E, Ben-Chetrit E, Caraco J, Rubinow A. Brucellosis in patients with heart disease: when should endocarditis be diagnosed? Cardiology. 1990; 77:313–317. PMID: 2073648.
Article20. Micozzi A, Venditti M, Gentile G, Alessandri N, Santero M, Martino P. Successful treatment of Brucella melitensis endocarditis with pefloxacin. Eur J Clin Microbiol Infect Dis. 1990; 9:440–442. PMID: 2387299.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Splenic Abscess Associated with Endocarditis in a Patient on Hemodialysis: A Case Report
- Successful Medical Treatment of Prosthetic Mitral Valve Endocarditis Caused by Brucella abortus
- A case of brucella endocarditis with spondylitis in a patient with multiple myeloma
- A Case of Spondylodiscitis with Spinal Epidural Abscess Due to Brucella
- A case of subacute infective endocarditis combined with multiple brain and splenic abscesses
