Diagnosis and Management of Congenital Coronary Arteriovenous Fistula in the Pediatric Patients Presenting Congestive Heart Failure and Myocardial Ischemia
- Affiliations
-
- 1Department of Pediatrics, Division of Pediatric Cardiology, Changhua Christian Hospital, Changhua, Taiwan. ferdielee@yahoo.com
- 2Center for Medical Genetics, Changhua Christian Hospital, Changhua, Taiwan.
- 3Department of Medical Genetics, College of Medicine and Hospital, National Taiwan University, Taipei, Taiwan.
- KMID: 1782974
- DOI: http://doi.org/10.3349/ymj.2009.50.1.95
Abstract
- PURPOSE
Four pediatric patients with congenital coronary arteriovenous fistula (CAVF) were reported to remind pediatric practitioners and cardiologists of its diagnosis and management.
MATERIALS AND METHODS
Four pediatric patients with congenital CAVF from June 1999 to November 2007 were included in this retrospective study. Study modalities included reviews of patients' profiles of clinical features, chest radiograph, Doppler echocardiography, cardiac catheterization with angiography, myocardial perfusion scan, and computed tomography.
RESULTS
All 4 patients were symptomatic. The clinical symptoms and signs were feeding problem, continuous murmur, tachycardia, tachypnea, cardiomegaly, and exertional chest pain. Myocardial enzyme was elevated in 1 patient. Echocardiography showed dilatation of the coronary artery in all 4 patients, and traced down its origin in 3 and drainage in 4. The fistulas originated from the right coronary artery in 2 patients and left coronary artery in 2, and were drained into the right ventricle in 2, right atrium in 1, and pulmonary artery in 1. Single left coronary artery was found in 1 patient. The pulmonary-to-systemic blood flow ratios ranged from 1.2 to 2.5. Transcatheter coil occlusion was successfully performed in 4 patients through a coaxial delivery system. The symptoms and signs of congestive heart failure and myocardial ischemia disappeared after the procedure.
CONCLUSION
Diagnosis of congenital CAVF could be achieved by appreciation of continuous murmur over area unusual for the ductus, and by scrupulous examination of echocardiography as well as angiography of the coronary artery through which coaxial transcatheter coil occlusion could be performed successfully.
Keyword
MeSH Terms
-
*Arteriovenous Fistula/complications/radiography/therapy
Child
Child, Preschool
Coronary Angiography
Coronary Circulation
*Coronary Vessel Anomalies/complications/radiography/therapy
*Embolization, Therapeutic
Female
*Heart Failure/etiology/radiography/therapy
Humans
Infant
Male
*Myocardial Ischemia/etiology/radiography/therapy
Figure
-
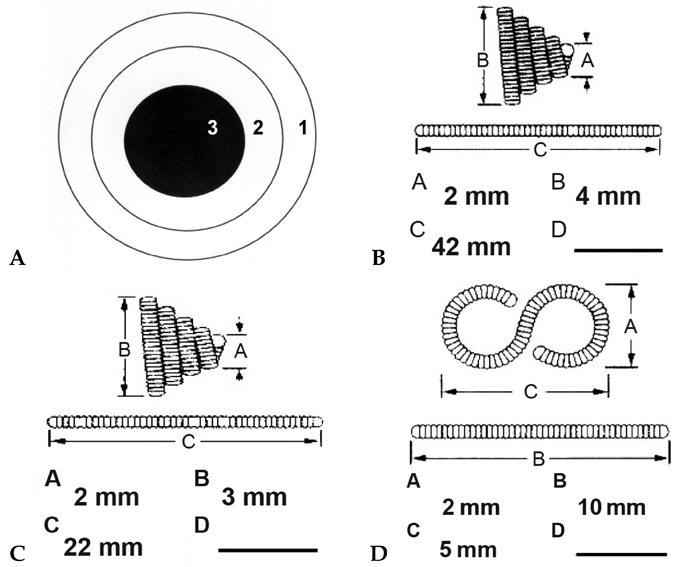
Fig. 1 (A) Cross section of the coaxial delivery system, which is composed of a strong "supportive catheter" of either 5-French Amplatz Right I Catheter or 5-French Judkins Coronary Catheter in the outer layer (denoted as Arabic numeral 1), a flexible "target-tracker catheter" of either 2.4-French Progreat or 2.5-French Tracker-18MX Infusion Catheter in the inner layer (denoted as Arabic numeral 2), and (B and C) cone-shaped Vortx-18 or (D) S-shaped Complex Helical Fibered Platinum Coil-18 followed by the Coil Pusher-16 in the central core (denoted as Arabic numeral 3). By means of this coaxial delivery system, two different modalities of Fibered Platinum Coil-18, which were chosen according to the geometry of fistula, could be steadily dislodged at the distal end by the Coil Pusher-16 through the flexible infusion catheter of "Progreat" or "Tracker-18MX" within the meandering congenital CAVF. CAVF, coronary arteriovenous fistula.
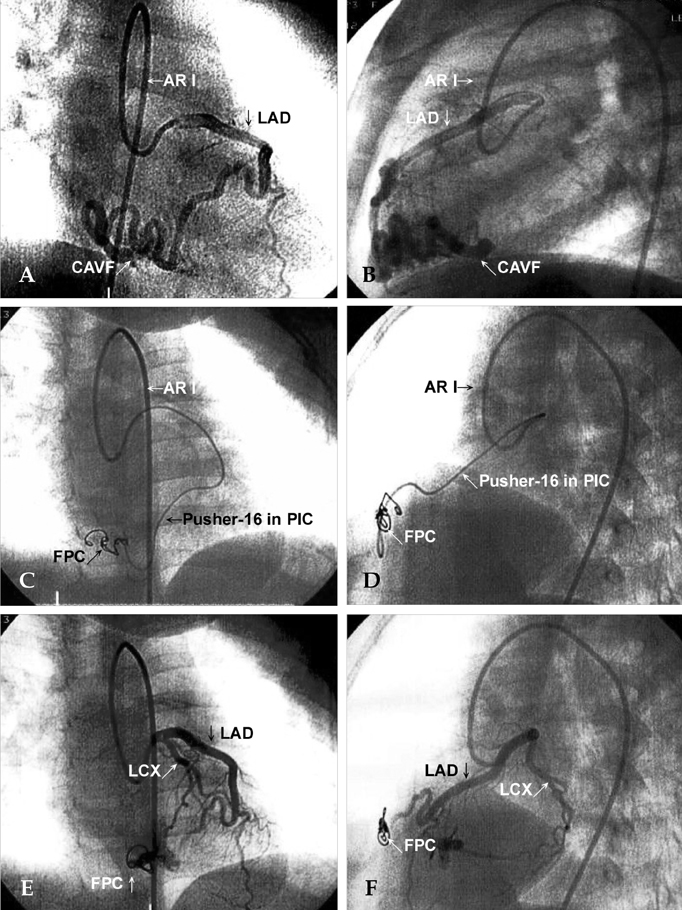
Fig. 2 (A and B) Selective angiography of the left coronary artery, which was entered by a 5-French Amplatz Right I (AR I), showed a single left coronary arteriovenous fistula (CAVF) originating from left anterior descending coronary artery (LAD) draining to the right ventricle. (C and D) With the aid of a rail offered by a 0.014-in PTCA Guide Wire, a 2.4-French Progreat Infusion Catheter (PIC), which was passed through a 5-French Amplatz Right I (AR I) that approached the left coronary artery at the orifice, tracked this meandering single left CAVF to the distal end. Transcatheter coaxial coil occlusion was performed, after removal of the 0.014-in guide wire, using a Vortx Coil Pusher-16 to dislodge 3 sets of 0.018-in Fibered Platinum Coil (FPC). (E and F) Selective angiography of the left coronary artery, 15 minutes. after coil occlusion, showed complete occlusion of the fistula and visualization of the left circumflex coronary artery (LCX), implying presence of insidious coronary artery steal phenomenon caused by this fistulous shunting.
Reference
-
1. Chu E, Cheitlin MD. Diagnostic considerations in patients with suspected coronary artery anomalies. Am Heart J. 1993. 126:1427–1438.2. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990. 21:28–40.
Article3. Roberts WC. Major anomalies of coronary arterial origin seen in adulthood. Am Heart J. 1986. 111:941–963.
Article4. Liberthson RR, Sagar K, Berkoben JP, Weintraub RM, Levine FH. Congenital coronary arteriovenous fistula. Report of 13 patients, review of the literature and delineation of management. Circulation. 1979. 59:849–854.
Article5. Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol. 2006. 107:7–10.
Article6. Kamiya H, Yasuda T, Nagamine H, Sakakibara N, Nishida S, Kawasuji M, et al. Surgical treatment of congenital coronary artery fistulas: 27 years' experience and a review of the literature. J Card Surg. 2002. 17:173–177.
Article7. Blanche C, Chaux A. Long-term results of surgery for coronary artery fistulas. Int Surg. 1990. 75:238–239.8. Bogers AJ, Quaegebeur JM, Huysmans HA. Early and late results of surgical treatment of congenital coronary artery fistula. Thorax. 1987. 42:369–373.
Article9. Urrutia-S CO, Falaschi G, Ott DA, Cooley DA. Surgical management of 56 patients with congenital coronary artery fistulas. Ann Thorac Surg. 1983. 5:300–307.10. Kung GC, Moore P, McElhinney DB, Teitel DF. Retrograde transcatheter coil embolization of congenital coronary artery fistulas in infants and young children. Pediatr Cardiol. 2003. 24:448–453.
Article11. Ogoh Y, Akagi T, Abe T, Hashino K, Hayabuchi N, Kato H. Successful embolization of coronary arteriovenous fistula using an interlocking detachable coil. Pediatr Cardiol. 1997. 18:152–155.
Article12. Beekman RH 3rd, Shim D, Lloyd TR. Embolization therapy in pediatric cardiology. J Interv Cardiol. 1995. 8:543–556.
Article13. De Wolf D, Terriere M, De Wilde P, Reidy JF. Embolization of a coronary fistula with a controlled delivery platinum coil in a 2-year-old. Pediatr Cardiol. 1994. 15:308–310.
Article14. Latson LA, Forbes TJ, Cheatham JP. Transcatheter coil embolization of a fistula from the posterior descending coronary artery to the right ventricle in a two-year-old child. Am Heart J. 1992. 124:1624–1626.
Article15. Perry SB, Rome J, Keane JF, Baim DS, Lock JE. Transcatheter closure of coronary artery fistulas. J Am Coll Cardiol. 1992. 20:205–209.
Article16. Reidy JF, Anjos RT, Qureshi SA, Baker EJ, Tynan MJ. Transcatheter embolization in the treatment of coronary artery fistulas. J Am Coll Cardiol. 1991. 8:187–192.
Article17. Moskowitz WB, Newkumet KM, Albrecht GT, Goble MM, Schieken RM. Case of steel versus steal: coil embolization of congenital coronary arteriovenous fistula. Am Heart J. 1991. 121:909–911.
Article18. Issenberg HJ. Transcatheter coil closure of a congenital coronary arterial fistula. Am Heart J. 1990. 120:1441–1443.
Article19. Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation. 1978. 58:25–34.
Article20. Gupta NC, Beauvais J. Physiologic assessment of coronary artery fistula. Clin Nucl Med. 1991. 16:40–42.
Article21. Lau G. Sudden death arising from a congenital coronary artery fistula. Forensic Sci Int. 1995. 73:125–130.
Article22. Sherwood MC, Rockenmacher S, Colan SD, Geva T. Prognostic significance of clinically silent coronary artery fistulas. Am J Cardiol. 1999. 83:407–411.
Article23. Vitarelli A, De Curtis G, Conde Y, Colantonio M, Di Benedetto G, Pecce P, et al. Assessment of congenital coronary artery fistulas by transesophageal color Doppler echocardiography. Am J Med. 2002. 113:127–133.
Article24. Sreedharan M, Prasad G, Barooah B, Dash PK. Vortex coil embolisation of coronary artery fistula. Int J Cardiol. 2004. 94:323–324.
Article25. Vance MS. Use of platinum microcoils to embolize vascular abnormalities in children with congenital heart disease. Pediatr Cardiol. 1998. 19:145–149.26. Olgunturk R, Kula S, Tunaoglu FS. Transcatheter closure of a rare form of coronary arteriovenous fistula (circumflex artery to coronary sinus). Int J Cardiol. 2006. 113:261–263.27. Papazoglou PD, Mitsibounas D, Nanas JN. Left anterior descending coronary artery-left ventricular fistula presenting as unstable angina and syncope. Int J Cardiol. 2004. 96:121–122.28. Mutlu H, Serdar-Küçükoğlu M, Ozhan H, Kansýz E, Oztürk S, Uner S. A case of coronary artery fistula draining into the pericardium causing hematoma. Cardiovasc Surg. 2001. 9:201–203.
Article29. Lee ML, Chaou WT, Wang YM, Fang W, Chiu IS. A new embryonic linkage between chromosome 22q11 deletion and a right ductus from a right aortic arch in a neonate with DiGeorge syndrome. Int J Cardiol. 2001. 79:315–316.
Article30. Currarino G, Willis K, Miller W. Congenital fistula between an aberrant systemic artery and a pulmonary vein without sequestration. A report of three cases. J Pediatr. 1975. 87:554–557.31. Lee ML, Wang JK, Wu MH, Chang CI, Lue HC. Echocardiographic and angiographic identification of ruptured sinus of Valsalva and aortic root abscess complicating infective endocarditis in ventricular septal defect: report of two cases. Acta Cardiol Sin. 1995. 11:87–91.32. Lee ML. Recognition of Berry syndrome in a 4-day-old neonate by echocardiography and transvenous angiocardiography. Int J Cardiol. 1999. 71:93–95.33. Lee ML, Wang JK, Lue HC. Visualization of pulmonary vein obstruction by pulmonary artery wedge injection and documentation by pressure tracings: report of one case with persistent wheezing following correction of total anomalous pulmonary venous connection. Int J Cardiol. 1995. 49:167–172.34. Lue HC, Sung TC, Hou SH, Wu MH, Cheng SJ, Chu SH, et al. Ventricular septal defect in Chinese with aortic valve prolapse and aortic regurgitation. Heart Vessels. 1986. 2:111–116.35. Velvis H, Schmidt KG, Silverman NH, Turley K. Diagnosis of coronary artery fistula by two-dimensional echocardiography, pulsed Doppler ultrasound and color flow imaging. J Am Coll Cardiol. 1989. 14:968–976.
Article36. Barbosa MM, Katina T, Oliveira HG, Neuenschwander FE, Oliveira EC. Doppler echocardiographic features of coronary artery fistula: report of 8 cases. J Am Soc Echocardiogr. 1999. 12:149–154.37. Cox ID, Heald SC, Murday AJ. Value of transoesophageal echocardiography in surgical ligation of coronary artery fistulas. Heart. 1996. 76:181–182.
Article38. Krishnamoorthy KM, Rao S. Transesophageal echocardiography for the diagnosis of coronary arteriovenous fistula. Int J Cardiol. 2004. 96:281–283.
Article39. Hofbeck M, Wild F, Singer H. Improved visualisation of a coronary artery fistula by the "laid-back" aortogram. Br Heart J. 1993. 70:272–273.
Article40. Yoshimura N, Hamada S, Takamiya M, Kuribayashi S, Kimura K. Coronary artery anomalies with a shunt: evaluation with electron-beam CT. J Comput Assist Tomogr. 1998. 22:682–686.
Article41. Ropers D, Moshage W, Daniel WG, Jessl J, Gottwik M, Achenbach S. Visualization of coronary artery anomalies and their anatomic course by contrast-enhanced electron beam tomography and three-dimensional reconstruction. Am J Cardiol. 2001. 87:193–197.
Article42. Pucillo AL, Schechter AG, Moggio RA, Kay RH, Baum SJ, Herman MV. MR imaging in the definition of coronary artery anomalies. J Comput Assist Tomogr. 1990. 14:171–174.
Article43. Taoka Y, Nomura M, Harada M, Mitani T, Endo J, Kondo Y, et al. Coronary-pulmonary artery fistulae depicted by multiplanar reconstruction using magnetic resonance imaging. Jpn Circ J. 1998. 62:455–457.
Article44. Umaña E, Massey CV, Painter JA. Myocardial ischemia secondary to a large coronary-pulmonary fistula-case report. Angiology. 2002. 53:353–357.45. Farooki ZQ, Nowlen T, Hakimi M, Pinsky WW. Congenital coronary artery fistulae: a review of 18 cases with special emphasis on spontaneous closure. Pediatr Cardiol. 1993. 14:208–213.
Article46. Said SA, Landman GH. Coronary-pulmonary fistula: long-term follow-up in operated and non-operated patients. Int J Cardiol. 1990. 27:203–210.
Article47. Sunder KR, Balakrishnan KG, Tharakan JA, Titus T, Pillai VR, Francis B, et al. Coronary artery fistula in children and adults: a review of 25 cases with long-term observations. Int J Cardiol. 1997. 58:47–53.48. Sato F, Koishizawa T. Stress/Rest 99mTc-MIBI SPECT and 123I-BMIPP scintigraphy for indication of surgery with coronary artery to pulmonary artery fistula. Int Heart J. 2005. 46:355–361.
Article49. Krabill KA, Hunter DW. Transcatheter closure of congenital coronary arterial fistula with a detachable balloon. Pediatr Cardiol. 1993. 14:176–178.50. Qureshi SA, Reidy JF, Alwi MB, Lim MK, Wong J, Tay J, et al. Use of interlocking detachable coils in embolization of coronary arterivenous fistulas. Am J Cardiol. 1996. 78:110–113.51. Thomson L, Webster M, Wilson N. Transcatheter closure of a large coronary artery fistula with the Amplatzer duct occluder. Catheter Cardiovasc Interv. 1999. 48:188–190.52. Fischer G, Apostolopoulou SC, Rammos S, Kiaffas M, Kramer HH. Transcatheter closure of coronary arterial fistulas using the new Amplatzer vascular plug. Cardiol Young. 2007. 17:283–287.
Article53. Holzer R, Waller BR 3rd, Kahana M, Hijazi ZM. Percutaneous closure of a giant coronary arteriovenous fistula using multiple devices in a 12-day-old neonate. Catheter Cardiovasc Interv. 2003. 60:291–294.54. Wax DF, MaGee AG, Nykanen D, Benson LN. Coil embolization of a coronary artery to pulmonary artery fistula from an antegrade approach. Cathet Cardiovasc Diagn. 1997. 42:68–69.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Bilateral Coronary to Pulmonary Artery Fistulas Associated With Severe Aortic Regurgitation
- Severe Form of Persistent Thebesian Veins Presenting as Ischemic Heart Disease
- Coronary-Bronchial Artery Fistula Manifested by Hemoptysis and Myocardial Ischemia in a Patient with Bronchiectasis
- A Case of Congenital Coronary Arteriovenous Fistula Presented as Congestive Heart Failure and Aortic Valve Infective Endocarditis
- Congenital Intracranial Pial Arteriovenous Fistula Complicated with Congestive Heart Failure in Neonate: A Case Report
