Transcatheter Closure of Fenestration with Detachable Coils After the Fontan Operation
- Affiliations
-
- 1Department of Pediatrics, Samsung Seoul Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. kis@smc.samsung.co.kr
- 2Department of Thoracic and Cardiovascular Surgery, Samsung Seoul Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1781906
- DOI: http://doi.org/10.3346/jkms.2006.21.5.859
Abstract
- We report our experience in 13 patients who underwent transcatheter closure of Fontan fenestration with the Cook(R) detachable coils. These patients underwent the extracardiac type Fontan operation with a short conduit fenestration (n=7) or lateral tunnel type with a punch-hole fenestration (n=6). Fenestration closure was done at the mean age of 5.1+/-2.4 yr, average of 32 months after the Fontan operation. We used one to three coils depending on the fenestration type, size, and residual shunt. Aortic oxygen saturations increased by an average of 5.4 (2-9)% and mean pressures in the Fontan circuit increased by an average of 2.1 (0-6) mmHg. During fol-low-up (median of 23 months), five patients (4 in extracardiac, 1 in lateral tunnel) had complete occlusion of the fenestration on echocardiography. There was no immediate or late complication. Transcatheter closure of fenestration in Fontan operation using the Cook(R) detachable coil is a safe and feasible technique. However, the coil was ineffective for closure of a punch-hole fenestration in the lateral tunnel type operation. In the conduit type fenestration, some modification of fenestration method instead of a short conduit for coil closure or use of new device is necessary to increase complete closure rate.
Keyword
MeSH Terms
Figure
-
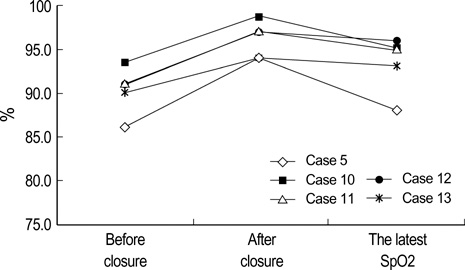
Fig. 1 Before and immediately after the fenestration closure and the latest systemic oxygen saturation in the patients with complete closure of fenestration.

Fig. 2 Before and immediately after the fenestration closure and the latest systemic oxygen saturation in the patients with incomplete closure of fenestration.

Fig. 3 Angiogram after fenestration closure in a patient who underwent lateral tunnel type Fontan operation. One loop of the coil is in the pulmonary atrial side, and the remained two loops are in the IVC-to-PA baffle. There is small residual shunt through the coil. IVC, inferior vena cava; PA, pulmonary artery.
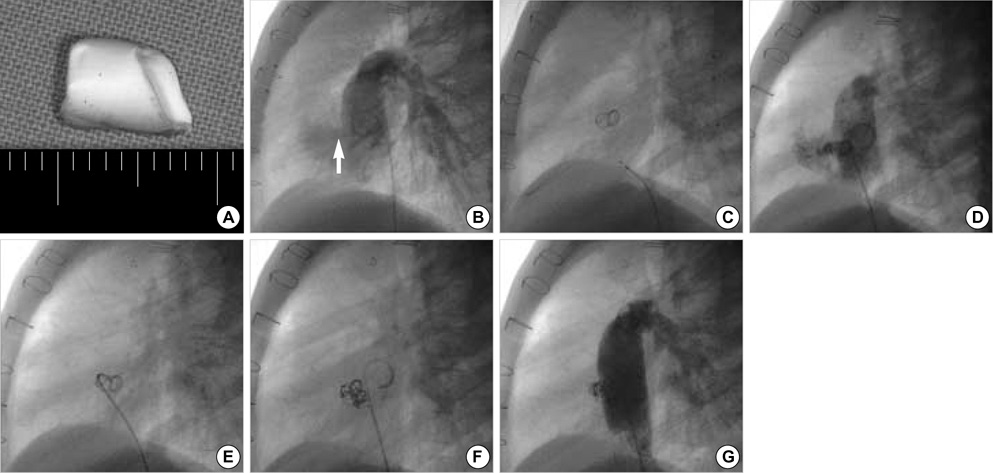
Fig. 4 Fenestration closure in a patient who underwent extracardiac type Fontan operation with a short conduit (A) as a fenestration. An angiogram shows the flow through this short conduit (B, arrow). There is small shunt on an angiogram (D) after the first coil detachment (C). Therefore we put the second (E) and the third coil (F) one by one. There is no significant residual fenestration flow after insertion of three coils (G).
Reference
-
1. de Leval MR, Kilner P, Gewillig M, Bull C. Total cavopulmonary connection: a logical alternative to atriopulmonary connection for complex Fontan operations. Experimental studies and early clinical experience. J Thorac Cardiovasc Surg. 1988. 96:682–695.2. Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax. 1971. 26:240–248.
Article3. Gundry SR, Razzouk AJ, del Rio MJ, Shirali G, Bailey LL. The optimal Fontan connection: a growing extracardiac lateral tunnel with pedicled pericardium. J Thorac Cardiovasc Surg. 1997. 114:552–558.
Article4. Marcelletti C, Corno A, Giannico S, Marino B. Inferior vena cavapulmonary artery extracardiac conduit. A new form of right heart bypass. J Thorac Cardiovasc Surg. 1990. 100:228–232.5. Bridges ND, Lock JE, Castaneda AR. Baffle fenestration with subsequent transcatheter closure. Modification of the Fontan operation for patients at increased risk. Circulation. 1990. 82:1681–1689.
Article6. Laks H, Pearl JM, Haas GS, Drinkwater DC, Milgalter E, Jarmakani JM, Isabel-Jones J, George BL, Williams RG. Partial Fontan: advantages of an adjustable interatrial communication. Ann Thorac Surg. 1991. 52:1084–1094.
Article7. Rosenthal DN, Friedman AH, Kleinman CS, Kopf GS, Rosenfeld LE, Hellenbrand WE. Thromboembolic complications after Fontan operations. Circulation. 1995. 92:II287–II293.
Article8. Cowley CG, Badran S, Gaffney D, Rocchini AP, Lloyd TR. Transcatheter closure of Fontan fenestrations using the Amplatzer septal occluder: initial experience and Follow-up. Catheter Cardiovasc Interv. 2000. 51:301–304.
Article9. Goff DA, Blume ED, Gauvreau K, Mayer JE, Lock JE, Jenkins KJ. Clinical outcome of fenestrated Fontan patients after closure: the first 10 years. Circulation. 2000. 102:2094–2099.10. Bridges ND, Lock JE, Mayer JE Jr, Burnett J, Castaneda AR. Cardiac catheterization and test occlusion of the interatrial communication after the fenestrated Fontan operation. J Am Coll Cardiol. 1995. 25:1712–1717.
Article11. Hijazi ZM. Extracardiac fenestrated Fontan operation: to close or not to close the fenestration? Catheter Cardiovasc Interv. 2001. 54:93–94.
Article12. Bradley TJ, Human DG, Culham JA, Duncan WJ, Patterson MW, LeBlanc JG, Sett SS. Clipped tube fenestration after extracardiac Fontan allows for simple transcatheter coil occlusion. Ann Thorac Surg. 2003. 76:1923–1928.
Article13. Sommer RJ, Recto M, Golinko RJ, Griepp RB. Transcatheter coil occlusion of surgical fenestration after Fontan operation. Circulation. 1996. 94:249–252.
Article14. Kim SJ, Lee JY, Song JY, Kim YH. Catheter closure of tube graft fenestration in extracardiac Fontan operation. Int J Cardiol. 2005. 104:224–226.
Article15. Rueda F, Squitieri C, Ballerini L. Closure of the fenestration in the extracardiac Fontan with the Amplatzer duct occluder device. Catheter Cardiovasc Interv. 2001. 54:88–92.
Article16. Moore JW, Murdison KA, Baffa GM, Kashow K, Murphy JD. Transcatheter closure of fenestrations and excluded hepatic veins after Fontan: versatility of the Amplatzer device. Am Heart J. 2000. 140:534–540.
Article17. Tofeig M, Walsh KP, Chan C, Ladusans E, Gladman G, Arnold R. Occlusion of Fontan fenestrations using the Amplatzer septal occluder. Heart. 1998. 79:368–370.
Article18. Mavroudis C, Zales VR, Backer CL, Muster AJ, Latson LA. Fenestrated Fontan with delayed catheter closure. Effects of volume loading and baffle fenestration on cardiac index and oxygen delivery. Circulation. 1992. 86:II85–II92.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Occlusion of the Patent Ductus Arteriosus with Cook Detachable Coil
- Treatment of Protein-losing Enteropathy After Fontan Procedure by Conversion to the Total Cavopulmonary Connection with Fenestration
- Three Cases of Hemolysis After Transcatheter Closure of A Patent Ductus Arteriosus
- Use of an Amplatzer Vascular Plug to occlude a tubular type of patent ductus arteriosus
- Comparison of Embolization Coils and Patent Ductus Arteriosus Occluders for Coronary Artery Fistula Transcatheter Closure: A Single Centre Experience
