Yonsei Med J.
2014 Jan;55(1):273-275. 10.3349/ymj.2014.55.1.273.
Renovascular Hypertension Treated by Renal Artery Embolization
- Affiliations
-
- 1Department of Pediatrics, Ajou University Hospital, Ajou University School of Medicine, Suwon, Korea. fli018@hanmail.net
- 2Department of Pediatrics, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1779917
- DOI: http://doi.org/10.3349/ymj.2014.55.1.273
Abstract
- Renovascular hypertension is caused by narrowing of the arteries supplying the kidneys. There are several methods to treat renal artery stenosis, such as medications, percutaneous transluminal renal angioplasty, and atherosclerosis. A boy presented to our hospital with severe hypertension. Computed tomography angiogram revealed severe narrowing of the left renal artery and hypoplastic left kidney. Total renal artery embolizaton was performed to make a complete occlusion of the left renal artery. Follow-up renin and aldosterone levels were gradually decreased. The main advantage of renal artery embolization is that it is minimally invasive compared with extensive surgical procedures. Therefore, renal artery embolization should be considered as an alternative to surgical nephrectomy in pediatric patients with renovascular hypertension.
MeSH Terms
Figure
-
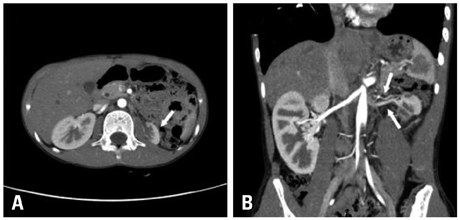
Fig. 1 Computed tomography, abdomen. Horizontal view (A) and coronal view (B) showing left renal arteries stenosis and hypoplastic left kidney (white arrows).
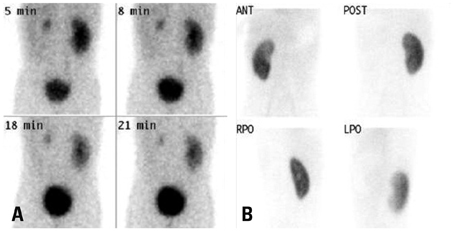
Fig. 2 Captopril-primed diethylene triamine pentaacetic acid scan (A) shows that the early uptake, perfusion, parenchymal transition time, and excretion were all delayed in the left kidney, as well as the decreased left kidney in size before embolization. 99 m Technetium-2, 3 dimercaptosuccinic acid scan (B) reveals no uptake in the left kidney, performed seven days after embolization.
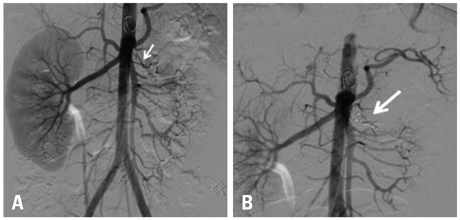
Fig. 3 Renovascular angiogram. Pre-embolization (A) and post-embolization (B) showing left renal artery stenosis, tortuous change, and total left renal arteries suppression.
Reference
-
1. Yerram P, Karuparthi PR, Chaudhary K. Pathogenesis and management of renovascular hypertension and ischemic nephropathy. Minerva Urol Nefrol. 2012; 64:63–72.2. Vogt B, Maillard M, Burnier M. Hypertension therapy in patients with renal artery stenosis. Ther Umsch. 2012; 69:279–281.3. Colyer WR, Eltahawy E, Cooper CJ. Renal artery stenosis: optimizing diagnosis and treatment. Prog Cardiovasc Dis. 2011; 54:29–35.
Article4. Capozza N, Collura G, Falappa P, Caione P. Renal embolization as an alternative to surgical nephrectomy in children. Transplant Proc. 2007; 39:1782–1784.
Article5. Reuter SR, Pomeroy PR, Chuang VP, Cho KJ. Embolic control of hypertension caused by segmental renal artery stenosis. AJR Am J Roentgenol. 1976; 127:389–392.
Article6. Ishijima H, Ishizaka H, Sakurai M, Ito K, Endo K. Partial renal embolization for pediatric renovascular hypertension secondary to fibromuscular dysplasia. Cardiovasc Intervent Radiol. 1997; 20:383–386.
Article7. Schwartz MJ, Smith EB, Trost DW, Vaughan ED Jr. Renal artery embolization: clinical indications and experience from over 100 cases. BJU Int. 2007; 99:881–886.
Article8. Docx MK, Vandenberghe P, Maleux G, Gewillig M, Mertens L. Severe hypertension due to renal polar artery stenosis in an adolescent treated with coil embolization. Pediatr Radiol. 2009; 39:1234–1237.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Renovascular Hypertension Controlled by Renal Artery Embolization
- A Case of Renal revascularization using Aortorenal Saphenous Vein Bypass Grafting in Renovascular Hypertension
- A Case of Curable Renovascular Hypertension Complicated by Renal Artery Embolism
- A Case of Renovascular Hypertension Controlled by Renal Autotransplantation
- A Case of Takayasu Arteritis with Renovascular Hypertension
