Gasless Transaxillary Robot-Assisted Neck Dissection: A Preclinical Feasibility Study in Four Cadavers
- Affiliations
-
- 1Department of Otolaryngology, School of Medicine, Ajou University, Suwon, Korea.
- 2Department of Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Korea. woungyounc@yuhs.ac
- 3Department of General Surgery, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Anatomy, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1779706
- DOI: http://doi.org/10.3349/ymj.2012.53.1.193
Abstract
- PURPOSE
We hypothesized that comprehensive neck dissection could be achieved via a gasless transaxillary approach using a robotic system. We intended to evaluate the accessibility of level I, IIB and VA nodes with transaxillary robot-assisted neck dissection of four cadavers.
MATERIALS AND METHODS
Transaxillary robotic neck dissection was performed in four cadavers through a 7-cm longitudinal incision at the anterior axilla and a 0.8-cm-sized incision in the chest wall.
RESULTS
We successfully performed neck dissection from level II to V in all four cadavers. However, dissection of levels IIB and VA, which lie on the cephalic portion of the spinal accessory nerve, was difficult. Vital structures, including the internal jugular vein, carotid artery, vagus nerve, phrenic nerve, superior thyroid artery and hypoglossal nerve, were successfully identified and preserved.
CONCLUSION
Our results demonstrate the feasibility of robot-assisted neck dissection using a transaxillary approach. We suggest that gasless, transaxillary robotic neck dissection is a promising technique for treating nodal metastasis in thyroid cancers or in selected squamous cell carcinomas of the head and neck. However, some modification of the approach might be needed when performing comprehensive neck dissections of all levels of the neck.
MeSH Terms
Figure
-

Fig. 1 Position and neck incision. With a cadaver placed in the supine position, the neck was slightly extended, and the dissection-side arm was abducted 45° and fixed; a 7 cm longitudinal skin incision along the anterior axillary line was made, and a second skin incision (0.8 cm long) was made on the medial side of the anterior chest wall.
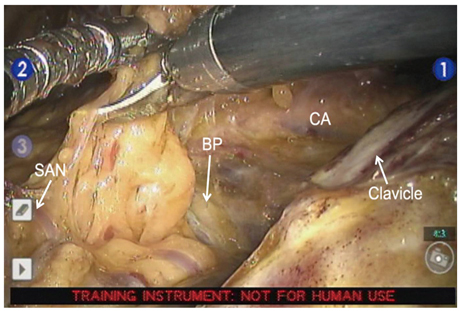
Fig. 2 Surgical view. SAN, spinal accessory nerve; BP, brachial plexus; CA, carotid artery.
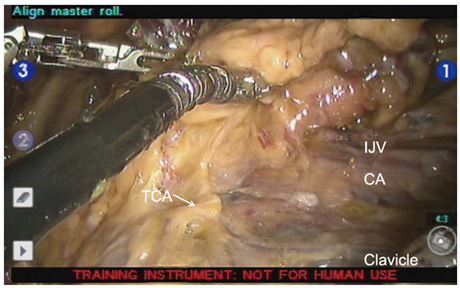
Fig. 3 Surgical view. TCA, transverse cervical artery; IJV, internal jugular vein, CA, carotid artery.

Fig. 4 Surgical view. STA, superior thyroid artery; digastric muscle, posterior belly of the digastric muscle; CA, carotid artery; IJV, internal jugular vein; SH, sternohyoid muscle.
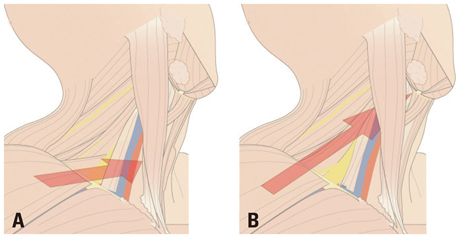
Fig. 5 The axis of robotic system (A) for level III, IV, V dissection; (B) for level II dissection.
Reference
-
1. Franklin ME Jr, Rosenthal D, Abrego-Medina D, Dorman JP, Glass JL, Norem R, et al. Prospective comparison of open vs laparoscopic colon surgery for carcinoma. Five-year results. Dis Colon Rectum. 1996. 39:S35–S46.2. Clinical Outcomes of Surgical Therapy Study Group. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med. 2004. 350:2050–2059.3. Weinstein GS, O'Malley BW Jr, Cohen MA, Quon H. Transoral robotic surgery for advanced oropharyngeal carcinoma. Arch Otolaryngol Head Neck Surg. 2010. 136:1079–1085.
Article4. Moore EJ, Olsen KD, Kasperbauer JL. Transoral robotic surgery for oropharyngeal squamous cell carcinoma: a prospective study of feasibility and functional outcomes. Laryngoscope. 2009. 119:2156–2164.
Article5. Park YM, Lee WJ, Lee JG, Lee WS, Choi EC, Chung SM, et al. Transoral robotic surgery (TORS) in laryngeal and hypopharyngeal cancer. J Laparoendosc Adv Surg Tech A. 2009. 19:361–368.
Article6. Park YM, Kim WS, Byeon HK, De Virgilio A, Jung JS, Kim SH. Feasiblity of transoral robotic hypopharyngectomy for early-stage hypopharyngeal carcinoma. Oral Oncol. 2010. 46:597–602.
Article7. Park YM, Lee JG, Lee WS, Choi EC, Chung SM, Kim SH. Feasibility of transoral lateral oropharyngectomy using a robotic surgical system for tonsillar cancer. Oral Oncol. 2009. 45:e62–e66.
Article8. Kang SW, Lee SC, Lee SH, Lee KY, Jeong JJ, Lee YS, et al. Robotic thyroid surgery using a gasless, transaxillary approach and the da Vinci S system: the operative outcomes of 338 consecutive patients. Surgery. 2009. 146:1048–1055.
Article9. Koh YW, Park JH, Kim JW, Lee SW, Choi EC. Endoscopic hemithyroidectomy with prophylactic ipsilateral central neck dissection via an unilateral axillo-breast approach without gas insufflation for unilateral micropapillary thyroid carcinoma: preliminary report. Surg Endosc. 2010. 24:188–197.
Article10. Kang SW, Lee SH, Ryu HR, Lee KY, Jeong JJ, Nam KH, et al. Initial experience with robot-assisted modified radical neck dissection for the management of thyroid carcinoma with lateral neck node metastasis. Surgery. 2010. 148:1214–1221.
Article11. Miccoli P, Berti P, Raffaelli M, Conte M, Materazzi G, Galleri D. Minimally invasive video-assisted thyroidectomy. Am J Surg. 2001. 181:567–570.
Article12. Ikeda Y, Takami H, Niimi M, Kan S, Sasaki Y, Takayama J. Endoscopic thyroidectomy by the axillary approach. Surg Endosc. 2001. 15:1362–1364.
Article13. Ballantyne GH, Moll F. The da Vinci telerobotic surgical system: the virtual operative field and telepresence surgery. Surg Clin North Am. 2003. 83:1293–1304.
Article14. Ferlito A, Rinaldo A, Silver CE, Gourin CG, Shah JP, Clayman GL, et al. Elective and therapeutic selective neck dissection. Oral Oncol. 2006. 42:14–25.
Article15. Shah JP. Patterns of cervical lymph node metastasis from squamous carcinomas of the upper aerodigestive tract. Am J Surg. 1990. 160:405–409.
Article16. Kim YH, Koo BS, Lim YC, Lee JS, Kim SH, Choi EC. Lymphatic metastases to level IIb in hypopharyngeal squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. 2006. 132:1060–1064.
Article17. Lim YC, Lee JS, Koo BS, Choi EC. Level IIb lymph node metastasis in laryngeal squamous cell carcinoma. Laryngoscope. 2006. 116:268–272.
Article18. Scheumann GF, Gimm O, Wegener G, Hundeshagen H, Dralle H. Prognostic significance and surgical management of locoregional lymph node metastases in papillary thyroid cancer. World J Surg. 1994. 18:559–567.
Article19. Koo BS, Yoon YH, Kim JM, Choi EC, Lim YC. Predictive factors of level IIb lymph node metastasis in patients with papillary thyroid carcinoma. Ann Surg Oncol. 2009. 16:1344–1347.
Article20. Witzel K, von Rahden BH, Kaminski C, Stein HJ. Transoral access for endoscopic thyroid resection. Surg Endosc. 2008. 22:1871–1875.
Article21. Song CM, Jung YH, Sung MW, Kim KH. Endoscopic resection of the submandibular gland via a hairline incision: a new surgical approach. Laryngoscope. 2010. 120:970–974.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Iatrogenic Horner’s Syndrome Developing after Robot-assisted Transaxillary Total Thyroidectomy
- Consideration of Complications after Gasless Transaxillary Endoscopic Thyroidectomy
- Comparison Study of Endoscopic Thyroidectomy Versus Robot-assisted Thyroidectomy by a Cervico-transaxillary Approach
- Use of the On-Q system for pain management after robot - assisted endoscopic transaxillary thyroidectomy
- Initial Experience Using Gasless Transaxillary Robotic Thyroidectomy by a Single Surgeon
