Yonsei Med J.
2007 Apr;48(2):247-254. 10.3349/ymj.2007.48.2.247.
Abduction Motion Analysis of Hemiplegic Shoulders with a Fluoroscopic Guide
- Affiliations
-
- 1Department of Rehabilitation Medicine, Ewha Womans University College of Medicine, Seoul, Korea.
- 2Department of Rehabilitation Medicine, The Catholic University of Korea, Daejeon, Korea. upperlimb@hanmail.net
- KMID: 1779527
- DOI: http://doi.org/10.3349/ymj.2007.48.2.247
Abstract
- PURPOSE
We investigated the usefulness of video based, fluoroscopically guided abduction motion analysis of hemiplegic shoulders. PATIENTS AND METHODS: Twenty-two stroke patients with Brunnstrom stages 3-4 (Group 1) or 5-6 (Group 2) were enrolled in this study. Patients with shoulder pain and significant spasticity (MAS 2) were excluded. We recorded motion pictures of the abductions of affected and unaffected shoulder joints under an AP fluoroscopic guide. Lateral scapular slide distances (D1: T2- superior angle, D2: T3- scapular spine, D3: T7-inferior angle) were measured at 30 degrees, 60 degrees, 90 degrees during glenohumeral abduction in a captured photographic image. The angles of scapular rotation and trajectory (stromotion) of the humeral head center, relative to the 3rd thoracic spine in the abduction motion were analyzed. RESULTS: In Group 1, a significant difference was found in the lateral scapular slide distance between the affected and sound sides. However, no significant side to side difference was found in Group 2. Scapular angles in abduction were also increased in Group 1. Patients with a more synergistic movement pattern showed less scapular stabilizing muscle activity and, instead, exhibited a compensatory "shrugging" like motion accomplished by spinal tilting. CONCLUSION: The present findings support the notion that the above parameters of fluoroscopically guided shoulder abduction motion analysis correlate well with clinical findings. These parameters should be useful for evaluations of hemiplegic shoulder biomechanics.
Keyword
MeSH Terms
Figure
-
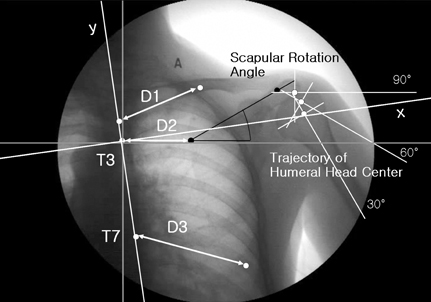
Fig. 1 Lateral scapular slide distance (D), scapular angle, trajectory of the center of the humeral head at 30° abduction in a right hemiplegic patient (image has been flipped for convenience) D, distance from the specific point from the medial border of scapular to the thoracic spine (D1, T2-Superior Angle; D2, T3-Scapular Spine; D3, T7-Inferior Angle) x, and y axes were reconstructed after considering tilting of the spine (white axis), original axis (grey line).
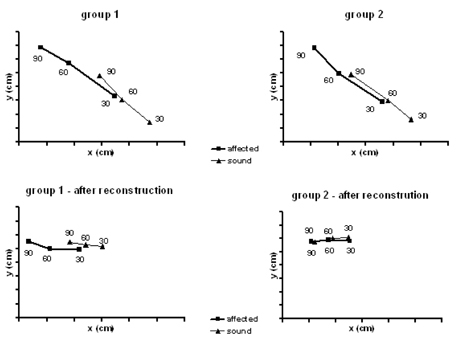
Fig. 2 Trajectory of the humeral head center at abduction. The lower two graphs show results after reconstructing the y axis after considering the effect of spinal tilting.
Reference
-
1. Turner-Stokes L, Jackson D. Shoulder pain after stroke: a review of the evidence base to inform the development of an integrated care pathway. Clin Rehabil. 2002. 16:276–298.2. Pandyan AD, Price CI, Rodgers H, Barnes MP, Johnson GR. Biomechanical examination of a commonly used measure of spasticity. Clin Biomech (Bristol, Avon). 2001. 16:859–865.3. Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med. 1998. 26:325–337.4. Endo K, Ikata T, Katoh S, Takeda Y. Radiographic assessment of scapular rotational tilt in chronic shoulder impingement syndrome. J Orthop Sci. 2001. 6:3–10.5. Poppen NK, Walker PS. Normal and abnormal motion of the shoulder. J Bone Joint Surg Am. 1976. 58:195–201.6. Van Ouwenaller C, Laplace PM, Chantraine A. Painful shoulder in hemiplegia. Arch Phys Med Rehabil. 1986. 67:23–26.7. Bohannon RW, Larkin PA, Smith MB, Horton MG. Shoulder pain in hemiplegia: statistical relationship with five variables. Arch Phys Med Rehabil. 1986. 67:514–516.8. Cheong JY, Shin HS, Han SJ, Hwang JH, Lee CK. Anterior displacement of humeral head in hemiplegic shoulder subluxation. J Korean Acad Rehab Med. 2002. 26:658–666.9. Shin JB, Kim SW, Park YS, Kim EH. Causes of the painful hemiplegic shoulder and comparison of the results of radiologic evaluation. J Korean Acad Rehab Med. 2003. 27:293–299.10. Hecht JS. Subscapular nerve block in the painful hemiplegic shoulder. Arch Phys Med Rehabil. 1992. 73:1036–1039.11. Cailliet R. Kaplan PE, Cailliet R, Kaplan CP, editors. Musculoskeletal manifestations of hemorrhagic stroke. Rehabilitation of stroke. 2003. 1st ed. Burlington (MA): Elsevier Science;103–128.12. Joynt RL. The source of shoulder pain in hemiplegia. Arch Phys Med Rehabil. 1992. 73:409–413.13. Kim SK, Lee KL, Han GS. Ultrasonographic evaluation of the painful hemiplegic shoulder. J Korean Acad Rehab Med. 1999. 23:622–629.14. Najenson T, Yacubovich E, Pikielni SS. Rotator cuff injury in shoulder joints of hemiplegic patients. Scand J Rehabil Med. 1971. 3:131–137.15. Lee KM, Lee JH, Park EH. The effect of subacromial massage for hemiplegic shoulder randomized controlled study. J Korean Acad Rehab Med. 2002. 26:385–390.16. Fu FH, Harner CD, Klein AH. Shoulder impingement syndrome. A critical review. Clin Orthop Relat Res. 1991. 269:162–173.17. Yoon YS, Jung SS, Lee KA, Kim JH, Lim JT. Assessment of shoulder subluxation using the lateral scapular slide test in hemiplegic patients. J Korean Acad Rehab Med. 2003. 27:819–823.18. Bagg SD, Forrest WJ. Electromyographic study of the scapular rotators during arm abduction in the scapular plane. Am J Phys Med. 1986. 65:111–124.19. Calliet R. The shoulder in hemiplegia. 1980. Philadelphia: FA Davis;55–72.20. Culham EG, Noce RR, Bagg SD. Shoulder complex position and glenohumeral subluxation in hemiplegia. Arch Phys Med Rehabil. 1995. 76:857–864.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Scapulohumeral Rhythm of Hemiplegic Patients by Plain X-ray Examination
- Effects of Intra-Articular Injection and Subscapularis Motor Point Block on Painful Hemiplegic Shoulder
- The Effect of Subacromial Massage for Hemiplegic Shoulder: Ramdomized Controlled Study
- Botulinum Toxin A Injection into the Subscapularis Muscle to Treat Intractable Hemiplegic Shoulder Pain
- Three-Dimensional Scapular Kinematics in Patients with Reverse Total Shoulder Arthroplasty during Arm Motion
