Yonsei Med J.
2006 Aug;47(4):513-518. 10.3349/ymj.2006.47.4.513.
Comparison of Clinical Characteristics Between Congenital Fiber Type Disproportion Myopathy and Congenital Myopathy with Type 1 Fiber Predominance
- Affiliations
-
- 1Department of Neurology, Konyang University College of Medicine, Daejeon, Korea.
- 2Department of Neurology, Brain Korea 21 Project for Medicine, Yonsei University College of Medicine, Seoul, Korea. ycchoi@yumc. yonsei.ac.kr
- 3Department of Rehabilitation Medicine, Brain Korea 21 Project for Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Pathology, Brain Korea 21 Project for Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 5Department of Neurology, Hallym University College of Medicine, Seoul, Korea.
- KMID: 1779501
- DOI: http://doi.org/10.3349/ymj.2006.47.4.513
Abstract
- Congenital myopathies are clinical and genetic heterogeneous disorders characterized by skeletal muscle weakness and specific structural changes in muscle fiber. Congenital myopathy with fiber type disproportion (CFTD) is an established disorder of congenital myopathy. CFTD is characterized by non-progressive childhood neuromuscular disorders with a relatively good prognosis and type 1 fiber predominance and smallness. Congenital myopathy with type 1 fiber predominance (CMT1P) is also a distinct entity of congenital myopathy characterized by non-progressive childhood neuromuscular disorders and type 1 fiber predominance without smallness. Little is known about CMT1P. Clinical characteristics, including dysmorphic features such as hip dislocation, kyphoscoliosis, contracture, and high arch palate, were analyzed along with laboratory and muscle pathologies in six patients with CMT1P and three patients with CFTD. The clinical manifestations of CFTD and CMT1P were similar. However, the frequency of dysmorphic features is less in CMT1P than in CFTD. Long term observational studies of CMT1P are needed to determine if it will change to another form of congenital myopathy or if CMT1P is a distinct clinical entity.
Keyword
MeSH Terms
Figure
-
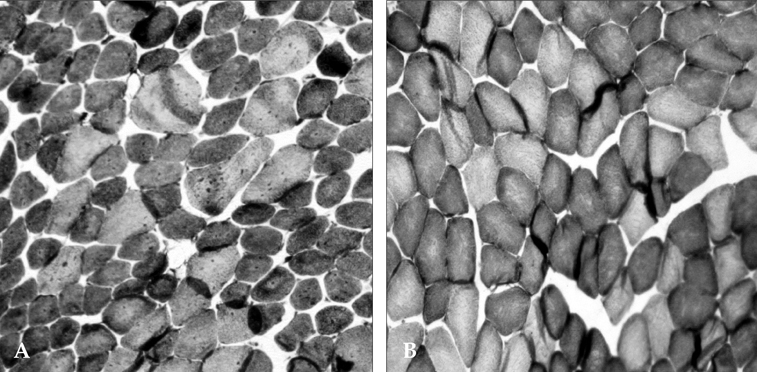
Fig. 1 The pathological findings of muscle biopsies for CFTD and CMT1P patients. Muscle biopsy shows type 1 fiber (dark fibers) predominance (> 55%) and relatively smaller (at least 12%) type 1 fibers compared to type 2 fibers (light fibers) (NADH-TR staining) (A). Muscle biopsy shows only type 1 fiber (dark fibers) predominance (> 55%) without other specific structural alterations. (NADH-TR staining) (B).
Reference
-
1. Bodensteiner JB. Congenital myopathies. Muscle Nerve. 1994. 17:131–144.2. Goebel HH. Congenital myopathies. Semin Pediatr Neurol. 1996. 3:152–161.3. Griggs RC, Mendell JR, Miller RG. Evaluation and treatment of myopathies. 1995. 1st ed. Philadelpia: Davis.4. Riggs JE, Bodensteiner JB, Schochet SS. Swaiman KF, Ashwal S, editors. Congenital myopathies. pediatric neurology: Principles and practice. 1999. 2nd ed. St. Louis: Mosby;1257–1263.5. Brooke MH. Kakulas BA, editor. Congenital fiber type disproportion. Clinical studies in myology. 1973. 1st ed. Amsterdam: Excerpta Medica;147–159.6. Brook MH. Brooke MH, editor. Congenital (more or less) muscle disease. A clinician's view of neuromuscular disease. 1986. 2nd ed. Baltimore: Williams & Wilkins;340–380.7. Dubowitz V. Dubowitz V, editor. Congenital myopathies. The Floppy Infant. 1980. 2nd ed. London: William Heinemann Medical;33–71.8. Brooke MH, Engel WK. The histographic analysis of human muscle biopsies with regard to fiber types. 4. Children's biopsies. Neurology. 1969. 19:591–605.9. Engel WK. Goldensohn ES, Appel SH, editors. Central core disease and focal loss of crosss-triation. Scientific approaches to clinical neurology. 1977. 1st ed. Philadelphia: Lea & Febiger;1555–1571.10. Engel WK. Goldensohn ES, Appel SH, editors. Rod (nemaline) disease. Scientific approaches to clinical neurology. 1977. 1st ed. Philadelphia: Lea & Febiger;1667–1691.11. Lambert CD. Uniform muscle histochemistry: a clinical and biopsy study. Trans Am Neurol Assoc. 1974. 99:120–125.12. Engel AG, Gomez MR, Groover RV. Multicore disease. A recently recognized congenital myopathy associated with multifocal degeneration of muscle fibers. Mayo Clin Proc. 1971. 46:666–681.13. Engel AG, Angelini C, Gomez MR. Fingerprint body myopathy: a newly recognized congenital muscle disease. Mayo Clin Proc. 1972. 47:377–387.14. Kyriakides T, Silberstein JM, Jongpiputvanich S, Silberstein EP, Walsh PJ, Gubbay SS, et al. The clinical significance of type 1 fiber predominance. Muscle Nerve. 1993. 16:418–423.15. Oh SJ, Danon MJ. Nonprogressive congenital neuromuscular disease with uniform type 1 fiber. Arch Neurol. 1983. 40:147–150.16. Nakagawa E, Ozawa M, Yamanouchi H, Sugai K, Goto Y, Nonaka I. Severe central nervous system involvement in a patient with congenital fiber-type disproportion myopathy. J Child Neurol. 1996. 11:71–73.17. Vestergaard H, Klein HH, Hansen T, Muller J, Skovby F, Bjorbaek C, et al. Severe insulin-resistant diabetes mellitus in patients with congenital muscle fiber type disproportion myopathy. J Clin Invest. 1995. 95:1925–1932.18. Cavanagh NP, Lake BD, McMeniman P. Congenital fibre type disproportion myopathy. A histological diagnosis with an uncertain clinical outlook. Arch Dis Child. 1979. 54:735–743.19. Banwell BL, Becker LE, Jay V, Taylor GP, Vajsar J. Cardiac manifestations of congenital fiber-type disproportion myopathy. J Child Neurol. 1999. 14:83–87.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Congenital Fiber Type Disproportion Associated with External Ophthalmoplegia
- Congenital Fiber Type Disproportion Myopathy: A case report
- Myopathy with Congenital Fiber Type Disproportion (CFTD): A case report
- Muscle fiber type disproportion with an autosomal dominant inheritance
- A Family of Congenital Fiber Type Disproportion with Mutation in Tropomyosin 3 (TPM3) Gene Presenting as Altered Mentality with Respiratory Distress
