Stroke from Delayed Embolization of Polymerized Glue Following Percutaneous Direct Injection of a Carotid Body Tumor
- Affiliations
-
- 1Department of Imaging Sciences and Interventional Radiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala, India. b_krish1@yahoo.co.in
- KMID: 1779443
- DOI: http://doi.org/10.3348/kjr.2007.8.3.249
Abstract
- A 52-year-old male with right carotid body tumor underwent direct percutaneous glue (n-butylcyanoacrylate [NBCA]) embolization. Several hours later, he developed left hemiparesis from embolization of the polymerized glue cast. Migration of glue during percutaneous tumor embolization is presumed to occur only in the liquid state, which may lead to stroke or cranial nerve deficits. To the best of our knowledge, this is the first report of delayed glue embolization from a treated hypervascular tumor of the head and neck.
Keyword
MeSH Terms
Figure
-
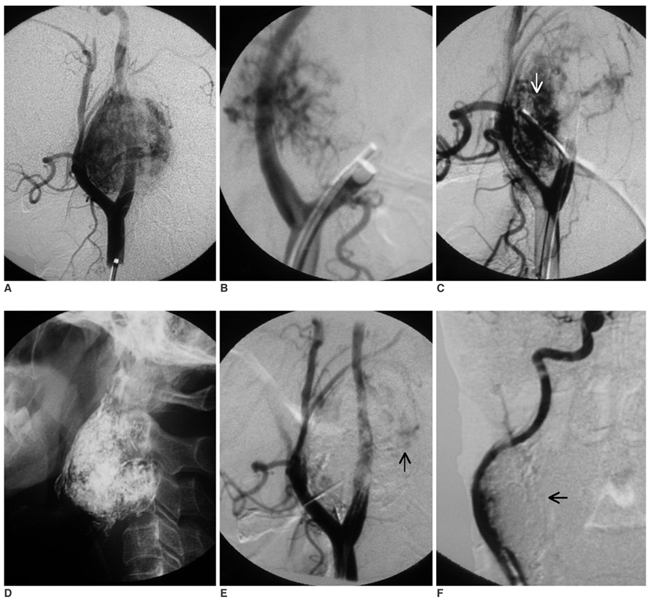
Fig. 1 A. Right carotid injection in the lateral view shows the hypervascular tumor with posterior displacement of the internal carotid artery. B. Oblique view of right carotid injection with balloon occlusion of the external carotid artery shows the feeder from the internal carotid artery. C. Balloon occlusion of the internal carotid artery with common carotid injection shows the residual vascular supply from the external carotid artery following embolization of the ascending pharyngeal artery. Note the tip of the needle for direct glue injection is well away from the internal carotid artery (arrow). D. Glue cast of the tumor after final embolization. E. Right common carotid injection in the lateral view at the end of the procedure shows near total devascularization of the tumor. A residual small area of tumor blush is seen posteriorly (arrow). Note the patent internal carotid artery flow. The overlying glue cast is mimicking artifactual filling defects in the internal carotid artery. F. Right common carotid injection in the oblique view clearly shows the internal carotid artery lumen is separate from the glue cast (arrow).
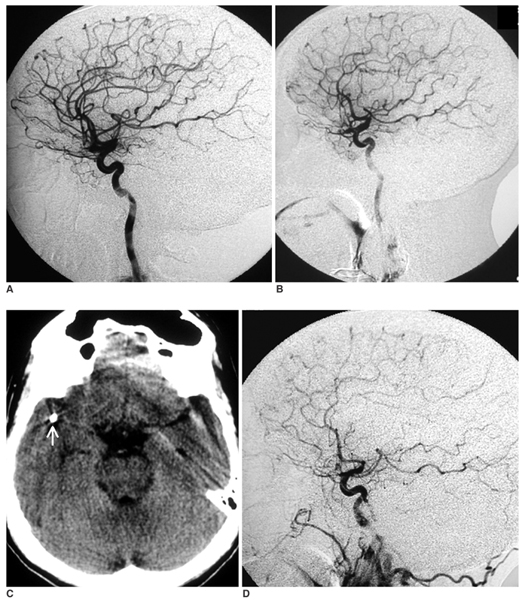
Fig. 2 A. Preprocedure right carotid injection in the lateral view shows the normal intracranial circulation. B. Immediate post procedure right carotid injection in the lateral view shows the preserved flow in all the cortical branches of the middle cerebral artery, including the rolandic and parietal branches. C. The non-enhanced CT scan of the brain at the level of the Circle of Willis shows the dense glue in the right sylvian fissure close to the location of the M2 segment (arrow). D. Right carotid lateral view six months later shows non-visualization of the rolandic and parietal branches of the middle cerebral artery, and this is suggestive of persistent occlusion.
Cited by 1 articles
-
A safer endovascular technique for pre-operative embolization of juvenile nasopharyngeal angiofibroma: avoiding the pitfalls of external carotid artery – internal carotid artery anastomoses
David Rosenbaum-Halevi, Victor Lopez-Rivera, Ali Turkmani, Aditya Sanzgiri, Hussein A. Zeineddine, Amber Luong, Peng Roc Chen
J Cerebrovasc Endovasc Neurosurg. 2020;22(2):97-105. doi: 10.7461/jcen.2020.22.2.97.
Reference
-
1. Casasco A, Herbreteau D, Houdart E, George B, Tran Ba Huy P, Deffresne D, et al. Devascularization of craniofacial tumors by percutaneous tumor puncture. AJNR Am J Neuroradiol. 1994. 15:1233–1239.2. George B, Casasco A, Deffrennes D, Houdart E. Intratumoral embolization of intracranial and extracranial tumors: technical note. Neurosurgery. 1994. 35:771–773.3. Valavanis A. Preoperative embolization of the head and neck: indications, patient selection, goals, and precautions. AJNR Am J Neuroradiol. 1986. 7:943–952.4. Abud DG, Mounayer C, Benndorf G, Piotin M, Spelle L, Moret J. Intratumoral injection of cyanoacrylate glue in head and neck paragangliomas. AJNR Am J Neuroradiol. 2004. 25:1457–1462.5. Horowitz M, Whisnant RE, Jungreis C, Snyderman C, Levy EI, Kassam A. Temporary balloon occlusion and ethanol injection for preoperative embolization of carotid-body tumor. Ear Nose Throat J. 2002. 81:536–538. 540542 passim6. Lonser RR, Heiss JD, Oldfield EH. Tumor devascularization by intratumoral ethanol injection during surgery. Technical note. J Neurosurg. 1998. 88:923–924.7. Harman M, Etlik O, Unal O. Direct percutaneous embolization of a carotid body tumor with n-butyl cyanoacrylate: an alternative method to endovascular embolization. Acta Radiol. 2004. 45:646–648.8. Liang Y, Wang D, Huang W, Ling F, Liu Y, Lu F. Direct intratumoral embolization of hypervascular tumors of the head and neck. Chin Med J. 2003. 116:616–619.9. Casasco A, Houdart E, Biondi A, Jhaveri HS, Herbreteau D, Aymard A, et al. Major complications of percutaneous embolization of skull-base tumors. AJNR Am J Neuroradiol. 1999. 20:179–181.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous N-Butyl Cyanoacrylate Embolization of a Pancreatic Pseudoaneurysm after Failed Attempts of Transcatheter Embolization
- Carotid Body Tumors
- Carotid Artery Reconstruction during the Resection of Carotid Body Tumor: A case report
- A Case of Pseudoaneurysm of the Supraorbital Artery Treated with Percutaneous Glue Embolization
- A Case of Carotid Body Tumor: Case Report
