Proactive Multifactorial Intervention Strategy Reduces the Risk of Cardiovascular Disease Estimated with Region-Specific Risk Assessment Models in Pacific Asian Patients Participating in the CRUCIAL Trial
- Affiliations
-
- 1Department of Cardiology, St Paul's Hospital, The Catholic University of Korea, Seoul, Korea. jhkim480kr@naver.com
- 2Pfizer Inc, New York, NY, USA.
- KMID: 1779414
- DOI: http://doi.org/10.3346/jkms.2013.28.12.1741
Abstract
- Despite race, ethnic, and regional differences in cardiovascular disease risk, many worldwide hypertension management guidelines recommend the use of the Framingham coronary heart disease (CHD) risk equation to guide treatment decisions. This subanalysis of the recently published CRUCIAL trial compared the treatment-related reductions in calculated CHD and stroke risk among Pacific Asian (PA) patients using a variety of region-specific risk assessment models. As a result, greater reductions in systolic and diastolic blood pressure, low-density lipoprotein cholesterol, and triglycerides were observed in the proactive multifactorial intervention (PMI) arm compared with the usual care arm at Week 52 for PA patients. The relative percentage change in 10-yr CHD risk between baseline and Week 52 in the PMI versus usual care arms was greatest using the NIPPON DATA80 fatal CHD model (LS [least square] mean difference -42.6%), and similar in the SCORE fatal CHD and Framingham total CHD models (LS mean difference -29.4% and -30.8%, respectively). The single-pill based PMI approach is consistently effective in reducing cardiovascular disease risk, evaluated using a variety of risk assessment models. (ClinicalTrials.gov registration number: NCT00407537)
Keyword
MeSH Terms
-
Adult
Age Factors
Aged
Asian Continental Ancestry Group/*statistics & numerical data
Blood Pressure
Cardiovascular Diseases/*etiology
Cholesterol, LDL/blood
Female
Follow-Up Studies
Humans
Hydroxymethylglutaryl-CoA Reductase Inhibitors/therapeutic use
Hypertension/diagnosis/drug therapy
Male
Middle Aged
Risk Assessment
Sex Factors
Treatment Outcome
Triglycerides/blood
Cholesterol, LDL
Hydroxymethylglutaryl-CoA Reductase Inhibitors
Triglycerides
Figure
-
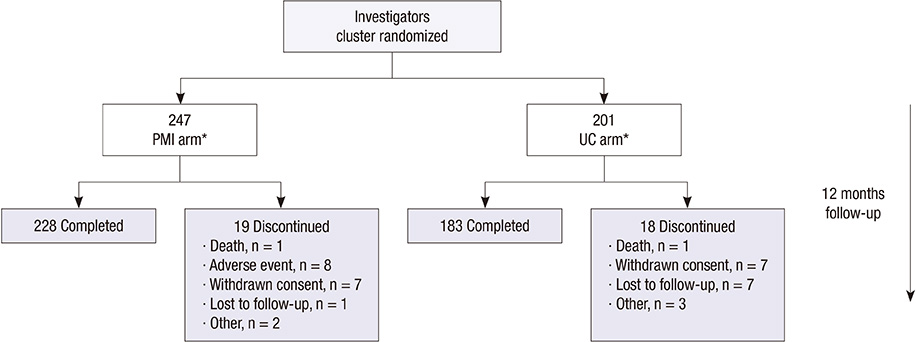
Fig. 1 Flow of PA patients through the CRUCIAL trial. *Treated patients with baseline and 1 or more post-baseline efficacy measurements. CRUCIAL, Cluster Randomized Usual Care versus Caduet Investigation Assessing Long-Term Risk; PA, Pacific Asian; PMI, proactive multifactorial intervention; UC usual care.
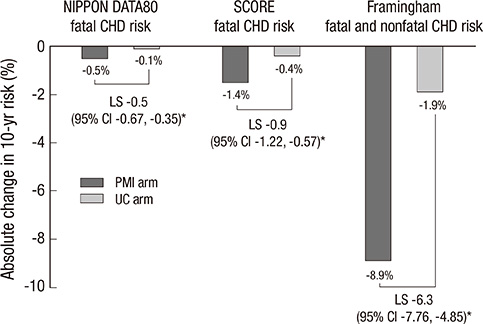
Fig. 2 Absolute percentage change in 10-yr CHD risk from baseline to Week 52 in each treatment arm among PA patients. *P < 0.001. CHD, coronary heart disease; CI, confidence interval; LS, least square mean for difference; NIPPON DATA80, National Integrated Project for Prospective Observation of Non-Communicable Disease and its Trends in the Aged, 1980; PMI, proactive multifactorial intervention; SCORE, Systematic Coronary Risk Evaluation; UC, usual care.
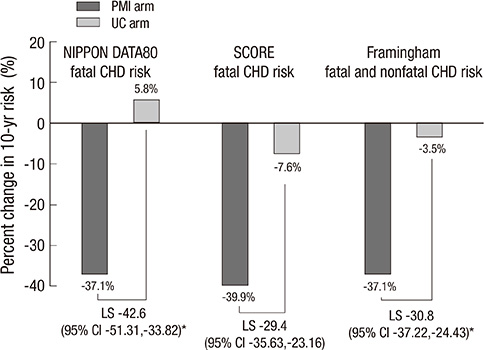
Fig. 3 Relative percentage change in 10-yr CHD risk from baseline to Week 52 by treatment arm among PA patients. *P < 0.001. CHD, coronary heart disease; CI, confidence interval; LS, least square mean for difference; NIPPON DATA80, National Integrated Project for Prospective Observation of Non-Communicable Disease and its Trends in the Aged, 1980; PMI, proactive multifactorial intervention; SCORE, Systematic Coronary Risk Evaluation; UC, usual care.
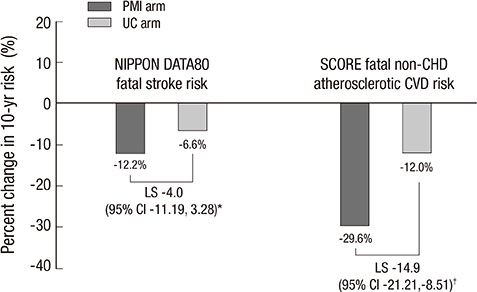
Fig. 4 Relative change in 10-yr fatal non-CHD risk from baseline to Week 52 by treatment arm among PA patients. *P = 0.283; †P < 0.001. CHD, coronary heart disease; CI, confidence interval; CVD, cardiovascular disease; LS, least square mean for difference; NIPPON DATA80, National Integrated Project for Prospective Observation of Non-Communicable Disease and its Trends in the Aged, 1980; PMI, proactive multifactorial intervention; SCORE, Systematic Coronary Risk Evaluation; UC, usual care.
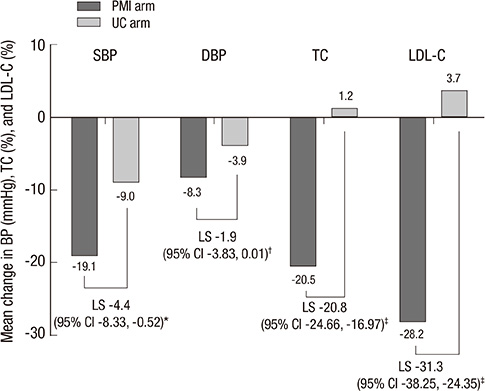
Fig. 5 Adjusted mean change from baseline in SBP and DBP (mmHg), and TC and LDL-C (%), from baseline to Week 52 by treatment arm among PA patients. *P < 0.05, †P = 0.051, ‡P < 0.001. CI, confidence interval; DBP, diastolic blood pressure; LDL-C, low-density lipoprotein cholesterol; LS, least square mean for difference; SBP, systolic blood pressure; TC, total cholesterol; PMI, proactive multifactorial intervention; UC, usual care.
Reference
-
1. Zamorano J, Erdine S, Pavia A, Kim JH, Al-Khadra A, Westergaard M, Sutradhar S, Yunis C. CRUCIAL Investigators. Proactive multiple cardiovascular risk factor management compared with usual care in patients with hypertension and additional risk factors: the CRUCIAL trial. Curr Med Res Opin. 2011; 27:821–833.2. Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation. 1998; 97:1837–1847.3. ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002; 288:2981–2997.4. Sever PS, Dahlöf B, Poulter NR, Wedel H, Beevers G, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial: Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet. 2003; 361:1149–1158.5. Lida M, Ueda K, Okayama A, Kodama K, Sawai K, Shibata S, Tanaka S, Keijnkai T, Horibe H, Minowa M, et al. Impact of elevated blood pressure on mortality from all causes, cardiovascular diseases, heart disease and stroke among Japanese: 14 year follow-up of randomly selected population from Japanese: Nippon data 80. J Hum Hypertens. 2003; 17:851–857.6. Zhou B, Zhang H, Wu Y, Li Y, Yang J, Zhao L, Zhang X. Ecological analysis of the association between incidence and risk factors of coronary heart disease and stroke in chinese populations. CVD Prevention. 1998; 1:207–216.7. Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: part II: variations in cardiovascular disease by specific ethnic groups and geographic regions and prevention strategies. Circulation. 2001; 104:2855–2864.8. Anand SS, Yusuf S, Vuksan V, Devanesen S, Teo KK, Montague PA, Kelemen L, Yi C, Lonn E, Gerstein H, et al. Differences in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada: the Study of Health Assessment and Risk in Ethnic groups (SHARE). Lancet. 2000; 356:279–284.9. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004; 364:937–952.10. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002; 106:3143–3421.11. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003; 42:1206–1252.12. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, et al. 2007 guidelines for the Management of Arterial Hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007; 25:1105–1187.13. D'Agostino RB Sr, Grundy S, Sullivan LM, Wilson P. CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. JAMA. 2001; 286:180–187.14. Conroy RM, Pyörälä K, Fitzgerald AP, Sans S, Menotti A, De Backer G, De Bacquer D, Ducimetière P, Jousilahti P, Keil U, et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. Eur Heart J. 2003; 24:987–1003.15. NIPPON DATA80 Research Group. Risk assessment chart for death from cardiovascular disease based on a 19-year follow-up study of a Japanese representative population. Circ J. 2006; 70:1249–1255.16. World Health Organization Regional Offices for South-East Asia and the Western Pacific. Chapter 8: priority noncommunicable diseases and conditions. Health in Asia and the Pacific. 2008.17. Wolf PA, D'Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: a risk profile from the Framingham Study. Stroke. 1991; 22:312–318.18. Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997; 349:1436–1442.19. Lee HS, Park YM, Kwon HS, Lee JH, Park YJ, Lim SY, Lee SH, Yoon KH, Son HY, Kim DS, et al. Prevalence, awareness, treatment, and control of hypertension among people over 40 years old in a rural area of South Korea: the Chungju Metabolic Disease Cohort (CMC) Study. Clin Exp Hypertens. 2010; 32:166–178.20. Wolf-Maier K, Cooper RS, Kramer H, Banegas JR, Giampaoli S, Joffres MR, Poulter N, Primatesta P, Stegmayr B, Thamm M. Hypertension treatment and control in five European countries, Canada, and the United States. Hypertension. 2004; 43:10–17.21. Lenfant C. Reflections on hypertension control rates: a message from the director of the National Heart, Lung, and Blood Institute. Arch Intern Med. 2002; 162:131–132.22. Brown BG, Stukovsky KH, Zhao XQ. Simultaneous low-density lipoprotein-C lowering and high-density lipoprotein-C elevation for optimum cardiovascular disease prevention with various drug classes, and their combinations: a meta-analysis of 23 randomized lipid trials. Curr Opin Lipidol. 2006; 17:631–636.23. Cannon CP, Steinberg BA, Murphy SA, Mega JL, Braunwald E. Meta-analysis of cardiovascular outcomes trials comparing intensive versus moderate statin therapy. J Am Coll Cardiol. 2006; 48:438–445.24. Steinhagen-Thiessen E, Bramlage P, Lösch C, Hauner H, Schunkert H, Vogt A, Wasem J, Jöckel KH, Moebus S. Dyslipidemia in primary care: prevalence, recognition, treatment and control: data from the German Metabolic and Cardiovascular Risk Project (GEMCAS). Cardiovasc Diabetol. 2008; 7:31.25. Lee J, Heng D, Chia KS, Chew SK, Tan BY, Hughes K. Risk factors and incident coronary heart disease in Chinese, Malay and Asian Indian males: the Singapore Cardiovascular Cohort Study. Int J Epidemiol. 2001; 30:983–988.26. Teo KK, Liu L, Chow CK, Wang X, Islam S, Jiang L, Sanderson JE, Rangarajan S, Yusuf S. INTERHEART Investigators in China. Potentially modifiable risk factors associated with myocardial infarction in China: the INTERHEART China Study. Heart. 2009; 95:1857–1864.27. Barzi F, Patel A, Gu D, Sritara P, Lam TH, Rodgers A, Woodward M. Cardiovascular risk prediction tools for populations in Asia. J Epidemiol Community Health. 2007; 61:115–121.28. Wu Y, Liu X, Li X, Li Y, Zhao L, Chen Z, Li Y, Rao X, Zhou B, Detrano R, et al. Estimation of 10-year risk of fatal and nonfatal ischemic cardiovascular diseases in Chinese adults. Circulation. 2006; 114:2217–2225.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The diversity of Fracture Risk Assessment Tool (FRAX)-based intervention thresholds in Asia
- Intensified Multifactorial Intervention in Patients with Type 2 Diabetes Mellitus
- Recent evidence on target blood pressure in patients with hypertension
- Asian Cohort Studies on Cardiovascular Risk Factors in Childhood
- A Comparison of KOSHA's Cardiovascular Disease Risk Assessment and the Predicted 10-year Risk of Cardiovascular Disease Developed by Jee for a Male Workers at a Wallpaper and Floor Covering Manufacturer
