J Korean Med Sci.
2011 Sep;26(9):1209-1213. 10.3346/jkms.2011.26.9.1209.
Influence of Diaphragmatic Mobility on Hypercapnia in Patients with Chronic Obstructive Pulmonary Disease
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Hospital, Gwangju, Korea. lscmd@jnu.ac.kr
- KMID: 1779396
- DOI: http://doi.org/10.3346/jkms.2011.26.9.1209
Abstract
- A reduction in diaphragm mobility has been identified in patients with chronic obstructive pulmonary disease (COPD) and has been associated with a decline in pulmonary function parameters. However, little information exists regarding the potential role of diaphragm mobility on hypercapnia in COPD. A new method of assessing the mobility of the diaphragm, using ultrasound, has recently been validated. The purpose of the present study was to investigate the relationship between diaphragm mobility and pulmonary function parameters, as well as that between arterial blood gas values and diaphragm mobility, in COPD patients. Thirty seven COPD patients were recruited for pulmonary function test, arterial blood gas analysis and diaphragm mobility using ultrasound to measure the craniocaudal displacement of the left branch of the portal vein. There were significant negative correlations between diaphragmatic mobility and PaCO2 (r = -0.373, P = 0.030). Diaphragmatic mobility correlated with airway obstruction (FEV1, r = 0.415, P = 0.011) and with ventilatory capacity (FVC, r = 0.302, P = 0.029; MVV, r = 0.481, P = 0.003). Diaphragmatic mobility also correlated significantly with pulmonary hyperinflation. No relationship was observed between diaphragm mobility and PaO2 (r = -0.028, P = 0.873). These findings support a possibility that the reduction in diaphragm mobility relates to hypercapnia in COPD patients.
MeSH Terms
-
Aged
Airway Resistance/physiology
Carbon Dioxide/blood/physiology
Diaphragm/physiopathology/*ultrasonography
Female
Humans
Hypercapnia/complications/*physiopathology
Male
Middle Aged
Portal Vein
Pulmonary Disease, Chronic Obstructive/complications/*physiopathology/ultrasonography
Pulmonary Gas Exchange
Respiratory Muscles/physiopathology
Figure
-
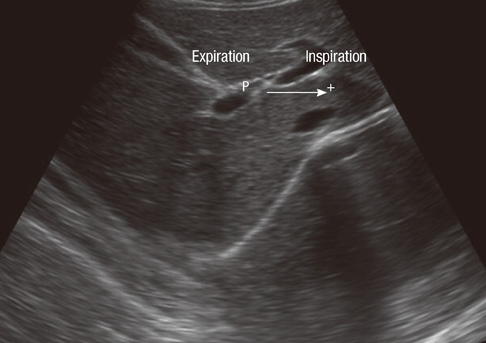
Fig. 1 B-mode ultrasonography measurement of craniocaudal displacement of the left intrahepatic portal vein branch. The line shows displacement of the left branch of the portal vein during maximal inspiratory and expiratory breathing in the sagittal plane. The P cursor marks the initial position of this vessel during maximal expiration, and another cursor (+) marks the position of the vessel during maximal inspiration. The craniocaudal displacement of this branch was recorded in millimeters.
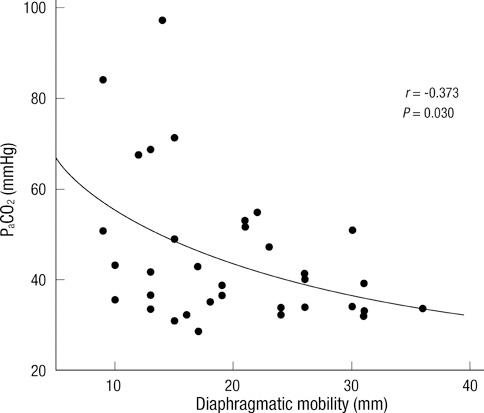
Fig. 2 The relationship between diaphragmatic mobility and the PaCO2. There was a negative linear correlation between the two measurements (r = -0.373, P = 0.030). PaCO2, arterial carbon dioxide tension.
Reference
-
1. Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, Fukuchi Y, Jenkins C, Rodriguez-Roisin R, van Weel C, Zielinski J. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007. 176:532–555.2. Iwasawa T, Kagei S, Gotoh T, Yoshiike Y, Matsushita K, Kurihara H, Saito K, Matsubara S. Magnetic resonance analysis of abnormal diaphragmatic motion in patients with emphysema. Eur Respir J. 2002. 19:225–231.3. Roussos C, Macklem PT. The respiratory muscles. N Engl J Med. 1982. 307:786–797.4. Rochester DF. The diaphragm: contractile properties and fatigue. J Clin Invest. 1985. 75:1397–1402.5. Dos Santos Yamaguti WP, Paulin E, Shibao S, Chammas MC, Salge JM, Ribeiro M, Cukier A, Carvalho CR. Air trapping: The major factor limiting diaphragm mobility in chronic obstructive pulmonary disease patients. Respirology. 2008. 13:138–144.6. Unal O, Arslan H, Uzun K, Ozbay B, Sakarya ME. Evaluation of diaphragmatic movement with MR fluoroscopy in chronic obstructive pulmonary disease. Clin Imaging. 2000. 24:347–350.7. Singh B, Eastwood PR, Finucane KE. Volume displaced by diaphragm motion in emphysema. J Appl Physiol. 2001. 91:1913–1923.8. Cassart M, Pettiaux N, Gevenois PA, Paiva M, Estenne M. Effect of chronic hyperinflation on diaphragm length and surface area. Am J Respir Crit Care Med. 1997. 156:504–508.9. Suga K, Tsukuda T, Awaya H, Takano K, Koike S, Matsunaga N, Sugi K, Esato K. Impaired respiratory mechanics in pulmonary emphysema: evaluation with dynamic breathing MRI. J Magn Reson Imaging. 1999. 10:510–520.10. Harris RS, Giovannetti M, Kim BK. Normal ventilatory movement of the right hemidiaphragm studied by ultrasonography and pneumotachography. Radiology. 1983. 146:141–144.11. Toledo NS, Kodaira SK, Massarollo PC, Pereira OI, Mies S. Right hemidiaphragmatic mobility: assessment with US measurement of craniocaudal displacement of left branches of portal vein. Radiology. 2003. 228:389–394.12. Houston JG, Fleet M, Cowan MD, McMillan NC. Comparison of ultrasound with fluoroscopy in the assessment of suspected hemidiaphragmatic movement abnormality. Clin Radiol. 1995. 50:95–98.13. West JB. Causes of carbon dioxide retention in lung disease. N Engl J Med. 1971. 284:1232–1236.14. Rochester DF, Braun NM. Determinants of maximal inspiratory pressure in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1985. 132:42–47.15. Gorini M, Spinelli A, Ginanni R, Duranti R, Gigliotti F, Scano G. Neural respiratory drive and neuromuscular coupling in patients with chronic obstructive pulmonary disease (COPD). Chest. 1990. 98:1179–1186.16. Toledo NS, Kodaira SK, Massarollo PC, Pereira OI, Mies S. Right hemidiaphragmatic mobility: assessment with US measurement of craniocaudal displacement of left branches of portal vein. Radiology. 2003. 228:389–394.17. McKenzie DK, Butler JE, Gandevia SC. Respiratory muscle function and activation in chronic obstructive pulmonary disease. J Appl Physiol. 2009. 107:621–629.18. Hoppin FG Jr. Theoretical basis for improvement following reduction pneumoplasty in emphysema. Am J Respir Crit Care Med. 1997. 155:520–525.19. Orozco-Levi M, Gea J, Lloreta JL, Félez M, Minguella J, Serrano S, Broquetas JM. Subcelullar adaptation of the human diaphragm in chronic obstructive pulmonary disease. Eur Respir J. 1999. 13:371–378.20. Gauthier AP, Verbanck S, Estenne M, Segebarth C, Macklem PT, Paiva M. Three-dimensional reconstruction of the in vivo human diaphragm shape at different lung volumes. J Appl Physiol. 1994. 76:495–506.21. Gross NJ. Extrapulmonary effects of chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2001. 7:84–92.22. Bégin P, Grassino A. Inspiratory muscle dysfunction and chronic hypercapnia in chronic obstructive pulmonary disease. Am Rev Respir Dis. 1991. 143:905–912.23. Zielinski J, MacNee W, Wedzicha J, Ambrosino N, Braghiroli A, Dolensky J, Howard P, Gorzelak K, Lahdensuo A, Strom K, Tobiasz M, Weitzenblum E. Causes of death in patients with COPD and chronic respiratory failure. Monaldi Arch Chest Dis. 1997. 52:43–47.24. Haluszka J, Chartrand DA, Grassino AE, Milic-Emili J. Intrinsic PEEP and arterial PCO2 in stable patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1990. 141:1194–1197.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Overlap Syndrome: Obstructive Sleep Apnea-Hypopnea Syndrome in Patients with Chronic Obstructive Pulmonary Disease
- The Study on the Effects of a Respiratory Rehabilitation Program for COPD Patients
- A Case of Acute Massive Pulmonary Emoblism Complicated by Hypercapnia
- Chronic Obstructive Pulmonary Disease: Respiratory Review of 2014
- Cor Pulmonale with Particular Reference to Chronic Obstructive Pulmonary Disease and Pulmonary Tuberculosis
