A Case of Histiocytic Sarcoma Presenting with Primary Bone Marrow Involvement
- Affiliations
-
- 1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. soleemd@amc.seoul.kr
- 2Department of Laboratory Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 1779267
- DOI: http://doi.org/10.3346/jkms.2010.25.2.313
Abstract
- Histiocytic sarcoma (HS) is a very rare neoplasm that often shows an aggressive clinical course and systemic symptoms, such as fever, weight loss, adenopathy, hepatosplenomegaly and pancytopenia. It may present as localized or disseminated disease. We describe here a 63-yr-old male who manifested systemic symptoms, including fever, weight loss and generalized weakness. Abdominal and chest computed tomography failed to show specific findings, but there was suspicion of multiple bony changes at the lumbar spine. Fusion whole body positron emission tomography, bone scan and lumbar spine magnetic resonance imaging showed multiple bone lesions, suggesting a malignancy involving the bone marrow (BM). Several BM and bone biopsies were inconclusive for diagnosis. Necropsy showed replacement of the BM by a diffuse proliferation of neoplastic cells with markedly increased cellularity (95%). The neoplastic cells were positive for lysozyme and CD68, but negative for T- and B-cell lineage markers, and megakaryocytic, epithelial, muscular and melanocytic markers. Morphologic findings also distinguished it from other dendritic cell neoplasms.
Keyword
MeSH Terms
-
Antigens, CD/metabolism
Antigens, Differentiation, Myelomonocytic/metabolism
Bone Marrow/metabolism/pathology
Bone Marrow Neoplasms/*diagnosis/pathology
Diagnosis, Differential
Histiocytic Sarcoma/*diagnosis/pathology
Humans
Magnetic Resonance Imaging
Male
Muramidase/metabolism
Positron-Emission Tomography
Tomography, X-Ray Computed
Antigens, CD
Antigens, Differentiation, Myelomonocytic
Muramidase
Figure
-
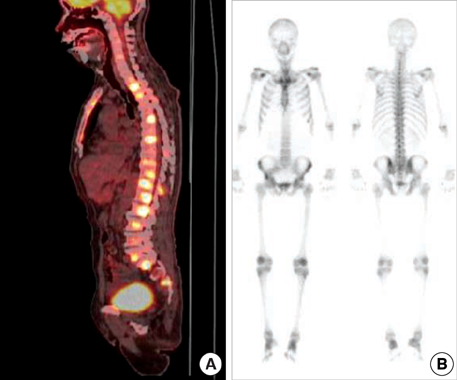
Fig. 1 Scanning findings for bones. (A) Disseminated hypermetabolic lesion (maxSUV=9.0, L2 body) at the whole spine by PET. A hypermetabolic lesion suggesting a primary malignant lesion was not detected in the lung, intraabdominal and pelvic organs. (B) No increased bone uptake of hypermetabolic lesions on bone scan, with little osteoblastic effect.

Fig. 2 Diffuse and heterogeneous T1 and T2 showing low SI changes in the lower thoracic and lumbar spine with subtle enhancement.

Fig. 3 Histopathological findings of bone marrow biopsy. (A) Non-cohesive proliferation of large pleomorphic neoplastic cells with large round-to-oval nuclei with vesicular chromatin and abundant foamy cytoplasm (H&E stain, ×400). Immunostaining with antibodies to (B) CD99, (C) CD68, (D) CD56, (E) HMB45 (each, ×100) and (F) S100 (×200).
Reference
-
1. Pileri SA, Grogan TM, Harris NL, Banks P, Campo E, Chan JK, Favera RD, Delsol G, De Wolf-Peeters C, Falini B, Gascoyne RD, Gaulard P, Gatter KC, Isaacson PG, Jaffe ES, Kluin P, Knowles DM, Mason DY, Mori S, Muller-Hermelink HK, Piris MA, Ralfkiaer E, Stein H, Su IJ, Warnke RA, Weiss LM. Tumours of histiocytes and accessory dendritic cells: an immunohistochemical approach to classification from the International Lymphoma Study Group based on 61 cases. Histopathology. 2002. 41:1–29.
Article2. Weiss LM, Grogan TM, Muller-Hermelink HK, Stein H, Dura WT, Favara B, Pauli M, Feller AC. Jaffe ES, Harris NL, Stein H, Vardiman JW, editors. Histiocytic sarcoma. WHO Classification of Tumors: Pathology and Genetics of Tumors of Haematopoietic and Lymphoid Tissues. 2001. 2nd ed. Lyon, France: IARC Press;278–279.3. Abidi MH, Tove I, Ibrahim RB, Maria D, Peres E. Thalidomide for the treatment of histiocytic sarcoma after hematopoietic stem cell transplant. Am J Hematol. 2007. 82:932–933.
Article4. Vos JA, Abbondanzo SL, Barekman CL, Andriko JW, Miettinen M, Aguilera NS. Histiocytic sarcoma: a study of five cases including the histiocyte marker CD163. Mod Pathol. 2005. 18:693–704.
Article5. Buonocore S, Valente AL, Nightingale D, Bogart J, Souid AK. Histiocytic sarcoma in a 3-year-old male: a case report. Pediatrics. 2005. 116:e322–e325.
Article6. Huang SC, Chang CL, Huang CH, Chang CC. Histiocytic sarcoma-a case with evenly distributed multinucleated giant cells. Pathol Res Pract. 2007. 203:683–689.7. Feldman AL, Minniti C, Santi M, Downing JR, Raffeld M, Jaffe ES. Histiocytic sarcoma after acute lymphoblastic leukaemia: a common clonal origin. Lancet Oncol. 2004. 5:248–250.
Article8. Alexiev BA, Sailey CJ, McClure SA, Ord RA, Zhao XF, Papadimitriou JC. Primary histiocytic sarcoma arising in the head and neck with predominant spindle cell component. Diagn Pathol. 2007. 2:7.9. Fukunaga M, Kato H. Histiocytic sarcoma associated with idiopathic myelofibrosis. Arch Pathol Lab Med. 2004. 128:1167–1170.
Article10. Kamel OW, Gocke CD, Kell DL, Cleary ML, Warnke RA. True histiocytic lymphoma: a study of 12 cases based on current definition. Leuk Lymphoma. 1995. 18:81–86.
Article11. Dalle JH, Leblond P, Decouvelaere A, Yakoub-Agha I, Preudhomme C, Nelken B, Mazingue F. Efficacy of thalidomide in a child with histiocytic sarcoma following allogeneic bone marrow transplantation for T-ALL. Leukemia. 2003. 17:2056–2057.12. Hornick JL, Jaffe ES, Fletcher CD. Extranodal histiocytic sarcoma: clinicopathologic analysis of 14 cases of a rare epithelioid malignancy. Am J Surg Pathol. 2004. 28:1133–1144.13. Carrasco DR, Fenton T, Sukhdeo K, Protopopova M, Enos M, You MJ, Di Vizio D, Nogueira C, Stommel J, Pinkus GS, Fletcher C, Hornick JL, Cavenee WK, Furnari FB, Depinho RA. The PTEN and INK4A/ARF tumor suppressors maintain myelolymphoid homeostasis and cooperate to constrain histiocytic sarcoma development in humans. Cancer Cell. 2006. 9:379–390.
Article14. Ralfkiaer E, Delsol G, O'Connor NT, Brandtzaeg P, Brousset P, Vejlsgaard GL, Mason DY. Malignant lymphomas of true histiocytic origin. A clinical, histological, immunophenotypic and genotypic study. J Pathol. 1990. 160:9–17.
Article15. Lauritzen AF, Delsol G, Hansen NE, Horn T, Ersboll J, Hou-Jensen K, Ralfkiaer E. Histiocytic sarcomas and monoblastic leukemias. A clinical, histologic, and immunophenotypical study. Am J Clin Pathol. 1994. 102:45–54.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bone marrow infiltration of histiocytic sarcoma
- A Case of Histiocytic Sarcoma Diagnosed by Bone Marrow Biopsy in a Patient Suffering from Fever for 8 Months
- Isolated Myeloid Sarcoma in the Nasal Cavity Without Bone Marrow Involvement in a 5-Year-Old Child
- Intraparenchymal Myeloid Sarcoma and Subsequent Spinal Myeloid Sarcoma for Acute Myeloblastic Leukemia
- A rare case of isolated myeloid sarcoma of the small gut with inv(16)(p13;q22) without bone marrow involvement
