J Korean Med Sci.
2011 Apr;26(4):580-582. 10.3346/jkms.2011.26.4.580.
A Case of Sheehan's Syndrome that Manifested as Bilateral Ptosis
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Dongguk University, Gyeongju, Korea. ysbae28@medimail.co.kr
- KMID: 1777892
- DOI: http://doi.org/10.3346/jkms.2011.26.4.580
Abstract
- Hypothyroidism can cause a variety of signs and symptoms of the neuromuscular system. However, ptosis in a patient with hypothyroidism is very rare. We report here on a case of central hypothyroidism that was due to Sheehan's syndrome and it manifested as bilateral ptosis in a 51-yr-old woman. She complained of exertional dyspnea and weakness. About 25-yr ago, she had a history of severe postpartum vaginal bleeding. The laboratory studies demonstrated hypopituitarism with secondary hypothyroidism. The ptosis was improved by replacement of thyroid hormone. Hypothyroidism should be considered in the differential diagnosis of patients who manifest with ptosis and that prompt replacement of hormone can lead to a complete recovery.
Keyword
MeSH Terms
-
Blepharoptosis/complications/*diagnosis/drug therapy
Electromyography
Female
Glucocorticoids/therapeutic use
Humans
Hypopituitarism/complications/*diagnosis/drug therapy
Hypothyroidism/complications
Magnetic Resonance Imaging
Middle Aged
Muscular Diseases/etiology
Neuromuscular Junction/physiopathology
Prednisolone/therapeutic use
Thyroxine/therapeutic use
Figure
-

Fig. 1 Bilateral ptosis before (A) and 3 months after (B) replacement of thyroid hormone.
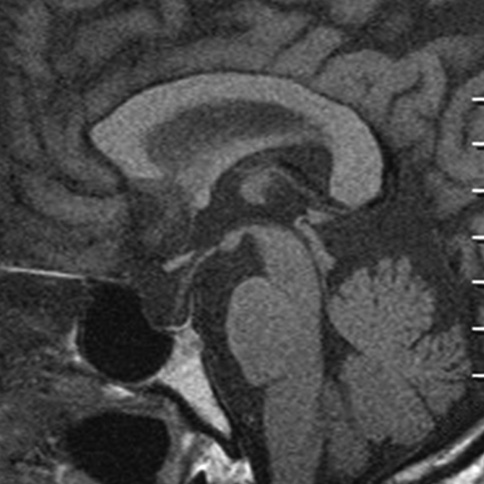
Fig. 2 The sagittal noncontrast T1 weighted magnetic resonance image of the brain shows an enlarged sella turcica and a nonvisualized gland.
Reference
-
1. Finsterer J. Ptosis: causes, presentation, and management. Aesthetic Plast Surg. 2003. 27:193–204.2. Penza P, Lombardi R, Camozzi F, Ciano C, Lauria G. Painful neuropathy in subclinical hypothyroidism: clinical and neuropathological recovery after hormone replacement therapy. Neurol Sci. 2009. 30:149–151.3. Green PH. Bilateral ptosis and proximal myopathy--muscular manifestations of hypothyroidism. Aust N Z J Med. 1977. 7:418–419.4. Lo YL, Ho SC, Koh LK, Khoo DH. EMG myokymia as a cause of ptosis in hypothyroidism. Eur J Neurol. 2003. 10:87–90.5. Narberhaus Donner B, Aguilar Cortés E, Playán Usón J, Berdún Chéliz MA, Bernat Badía A. Third cranial nerve paralysis associated with hypothyroidism. J Neurol. 1992. 239:176–177.6. Keleştimur F. Sheehan's syndrome. Pituitary. 2003. 6:181–188.7. Conti-Fine BM, Milani M, Kaminski HJ. Myasthenia gravis: past, present, and future. J Clin Invest. 2006. 116:2843–2854.8. Somay G, Oflazoğlu B, Us O, Surardamar A. Neuromuscular status of thyroid diseases: a prospective clinical and electrodiagnostic study. Electromyogr Clin Neurophysiol. 2007. 47:67–78.9. Cho WJ, Joo SP, Kim TS, Seo BR. Pituitary apoplexy presenting as isolated third cranial nerve palsy with ptosis: two case reports. J Korean Neurosurg Soc. 2009. 45:118–121.10. Kisakol G, Tunc R, Kaya A. Rhabdomyolysis in a patient with hypothyroidism. Endocr J. 2003. 50:221–223.11. Mor F, Green P, Wysenbeek AJ. Myopathy in Addison's disease. Ann Rheum Dis. 1987. 46:81–83.12. Kendall-Taylor P, Turnbull DM. Endocrine myopathies. Br Med J (Clin Res Ed). 1983. 287:705–708.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Sheehan's Syndrome with Pancytopenia
- The Effect of Elastic Eyelid Band Application on Bilateral Severe Ptosis in a Patient With Bilateral Incomplete Claude’s Syndrome: A Case Report
- A case of Sheehan's syndrome with central diabetes insipidus showing hemorrhagic pituitary apoplexy
- Case of Sheehan's Syndrome Misdiagnosed as Pituitary Apoplexy due to Pituitary Adenoma
- Management of Severe Bilateral Ptosis in a Patient With Midbrain Infarction: A Case Report
